Nutritional Status among the Women and Children in Bangladesh: Implications for Health Social Work Practice
Hanumant Waghmare, Hemvati Nandan Bahuguna Garhwal University
Sudhir Maske, Delhi University
Pooja Gaigaware, Tata Institute of Social Sciences
Abstract: Undernutrition is a serious public health concern in several Asian countries, especially in Bangladesh. This paper presents the findings of a study conducted to identify the factors influencing the nutritional status of women and children under the age of five, using data from the Demographic Health Survey. The study also explores potential social work interventions to address these issues through civil society and advocacy efforts. Despite government initiatives, the nutritional status of women and children remains a major concern in Bangladesh. The study assesses the nutritional status of women based on their Body Mass Index (BMI) and reports a decrease in the prevalence of anemia by 15.4% among women and 32.2% among children. Furthermore, the study indicates that nutritional policies and programs have had a positive impact on the nutritional status of women and children. The findings highlight the necessity of a robust support system that prioritizes a multi-sectoral approach to address undernutrition. The study emphasizes the importance of collective and coordinated efforts for the successful implementation of nutritional policies. Additionally, the study stresses the significance of understanding and perspectives about nutrition for social work researchers and practitioners to effectively address health-centered social work practices. Ultimately, the study underscores the direct link between health and nutrition and the broader goals of human well-being, inclusive, and sustainable development.
Keywords: Anemia; Nutritional Status; Women and Children; Social work Intervention
Introduction
The lack of proper nutrition can lead to both communicable and non-communicable diseases and can also reduce the work efficiency of women. According to the 2020 Global Nutrition Report, malnutrition affected 820 million people worldwide in 2015. Social workers have historically not been involved in discussing nutrition with their clients due to its technical nature, but it's crucial for them to understand how it contributes to marginalization and impacts human development. Nutrition plays a critical role in enhancing the cognitive and mental growth of a child. Given the increasing complexity of nutrition information and its impact on overall well-being, it's important for social workers to develop a deeper understanding of nutrition to better assess their clients' needs and implement effective interventions (Findley PA., 2020). Factors such as famine, natural disasters, civil wars, and reduced agricultural food production contribute to malnutrition. In Bangladesh, a decline in cultivation land, unequal income distribution, high product prices, and a large population dependent on seasonal occupations contribute to poor health indicators (Hossain M., 2005; Adams, et al. 2014; Raihan, M. J., Shamim, A. A., et al. 2017). Social workers in Bangladesh are playing a significant role in addressing nutrition concerns and are employing various strategies to strengthen nutrition services for women and children. Their interventions have led to improvements in food security by increasing food grain production, particularly rice, enhancing infrastructure, improving food delivery to the poor, and liberalizing agricultural input and output markets. Despite these efforts, Bangladesh remains one of the poorest and most climatically vulnerable countries and experiences a high prevalence of stunting and wasting among young children (Magnani, Oot, Sethuraman, Kabir, & Rahman, 2015; Hossain, M. A., Ahmed, F., et al. 2014; Tharakan, K. R. & Suchindran, P. S., 1999). Malnutrition rates in Bangladesh are some of the highest globally. More than half of women suffer from chronic energy deficiency, and studies suggest that there has been little improvement in women's nutritional status over the past 20 years (Ahmed, S. M., et al. 1998). . Consequently, around 54% of preschool-age children, equivalent to more than 9.5 million children, are stunted, while 56% are underweight, and around 17% are wasted. Malnutrition among women is also extremely prevalent in Bangladesh. As a matter of fact, maternal undernourishment is 38 % among women 15 to 19 years of age who have had a birth in the past 3 years. This underlies high levels of low birth weight (22%), stunting (41% under 5), and wasting (16% under 5) in Bangladesh (Chaparro, Oot, & Sethuraman, 2014).
The nutrition policy of Bangladesh was developed to combat both undernutrition and overnutrition. Undernutrition encompasses protein-energy Malnutrition and a deficiency of minerals, essential vitamins, and micronutrients (Ahmed et al., 2012, Gautham, et al. 015). Anaemia affects over two-thirds of children and under two-and-a-half of pregnant women. In Bangladesh, undernutrition continues to be a serious public health problem. Although overnutrition is still not a large problem, the prevalence of overweight among under-five children and women is increasing (Chaparro, Oot, & Sethuraman, 2014). Numerous regional studies have examined the nutrition status of women, but evidence of a national representative is lacking. This study examines prevalence and determinants of nutritional status among the women and children: Implications to health social work in Bangladesh by using a demographic health survey.
Materials and Methods: The present study utilizes the most recent Demographic Health Survey (DHS) data from Bangladesh 2014 (BDHS-7). The DHS is recognized as a nationally representative sample, covering diverse samples from across the country using a well-defined sampling procedure. The DHS employs a multi-stage stratified sampling method for sample selection. The survey gathers information on reproductive and child health, family planning, fertility, water and sanitation, nutrition, lifestyle, violence, and other topics using the prescribed DHS questionnaire format with some country-specific adjustments. A total of 7,300 households and 17,863 eligible women were interviewed during the survey. For the current study, only the household and eligible women's schedules are used for the analysis. Additionally, anthropometric parameters (height and weight) of women and children were collected during the survey. The anthropometric measurements included height and weight measurements for ever-married women aged 15-49 years and children under 5 years of age.
Variable description: This study is focused on the nutritional status of women aged 15-49 years and children under 5 years old in Bangladesh. The nutritional status of women is assessed using the body mass index (BMI), which is divided into four categories: underweight, normal weight, overweight, and obese. For children, nutritional status is determined by Z-scores for three parameters: stunting, wasting, and underweight & overweight for age. Stunting is categorized as severe or moderate, wasting is categorized as severe, moderate, or overweight, and weight for age is categorized as severe underweight, moderate underweight, or overweight (Arnold, Nangia, & Kapil, 2004).
Women nutritional status
Cut-off limit for BMI (Weight for Height)
· Underweight: BMI<18.5 kg/m2,
· Normal weight: 18.5≤BMI<24.9 kg/m2,
· Overweight: 24.9≤BMI<30.0 <kg/m2,
· Obese: BMI≥30.0 kg/m2
Children nutritional status
Cut-off limit for Stunting (Height-for-Age)
· Severely Stunted: Z-score <-3.0 SD below mean
· Moderately Stunted: Z-score <-2.0SD below mean
Cut-off limit for Wasting (Weight-for-Height)
· Severely Wasted: Z-score <-3.0 SD below mean
· Moderately Wasted: Z-score <-2.0 SD below mean
· Overweight: Z-score: > +2.0 SD below mean
Cut-off limit for Underweight (Weight-for-age)
· Severely underweight: Z-score < -3.0 SD below mean
· Moderately underweight: Z-score < -2.0 SD below mean
· Overweight: Z-score: > +2.0 SD below mean
Independent variables: Socio-economic and demographic characteristics of women and children are considered to understand the nutritional status by selected background characteristics. The selected socio-economic and demographic characteristics include: the place of residence (Rural, Urban), religion (Hindu, Muslim, Others), age (continuous), marital status (Married, Unmarried, Others), educational attainment, working status (Yes, No), Source of drinking water, type of cooking fuel, type of toilet facility, and wealth index. Apart from the above-mentioned variables, several children and dietary pattern (food composition) of women is considered and for children number of siblings, sex, breastfeeding pattern, immunization, and the dietary pattern were considered in the analysis. Descriptive statistics and bivariate analysis have been used to study the nutritional status among women aged 15-49 and children aged 0-59 months.
Methods
To determine factors associated with Body Mass Index among women, a multinomial logistic regression model was used. This allowed us to assess the independent effect of background characteristics in determining the prevalence of BMI. Multinomial logistic regression is an expansion of logistic regression in which one equation is set up for each logit relative to the reference outcome. BMI consist of four categories: normal, underweight, overweight, and obese. For a dependent variable with four categories, this requires the estimation of three equations, one for each category relative to the reference category (not related), to describe the relationship between the dependent and the independent variables:
ln [{P(Yi = 2)|Xi}/{P(Yi = 1)|Xi}] = α2 + β12X1 . . . βk2Xik ………1
ln [{P(Yi = 3)|Xi}/{P(Yi = 1)|Xi}] = α3 + β13X1 . . . βk3Xik ………..2
ln [{P(Yi = 4)|Xi}/{P(Yi = 1)|Xi}] = α4 + β14X1 . . . βk4Xik…...…....3
Where α2, α3, and α4 are the intercepts for the category underweight, overweight, and obese, respectively, and βk2, βk3, and βk4 are the slope coefficient of the Xi variables for the respective category of the dependent variable. We also used binary logistic regression to determine the factors associated with severe and moderate stunting, severe and moderate wasting, and severe and moderate underweight among children aged 0-59 months. In this analysis, the response variable 'no' was recoded as 0 if the child was not malnourished and, and 1 if a child was malnourished: loge [P(Yi = 1| Xi) / 1 – P(Yi = 1| Xi)] = = α + β1Xi1, . . . , βk Xik …..4
Where, Yi is the binary response variable; Xi is the set of explanatory variables, such as sociodemographic characteristics as mentioned in the case of the multinomial model; and β1, . . . , βk are the coefficients of the Xi variables.
Results
Profile of the study population: In Table 1, it is shown that 18.18% of women aged 15-49 were undernourished, while 19.19% were overweight. Among underweight women, the majority were in the 15-19 age group (28.38%). The prevalence of underweight (BMI <18.5 kg/m2) was higher in rural women compared to urban women (20.92% in rural areas vs 11.99% in urban areas). Conversely, the prevalence of overweight, according to WHO standards, was higher in urban areas compared to rural areas (27.35% vs 15.98%). The highest percentage of underweight women fell under the uneducated category (23.76%). The nutritional status of women was influenced by household facilities and lifestyle. Specifically, underweight women were found in households with water supply from unprotected wells and among those who used agricultural waste as cooking fuel. Comparing overweight women (BMI>=30.0 & <29.9 kg/m2) according to the head of the household, women in female-headed households had a higher percentage of overweight individuals compared to male-headed households (21.04% vs 18.96%). In terms of wealth index, a higher proportion of underweight women were from the poorest households as opposed to the richest households (30.96% vs 7.02%).
Table 1: Percentage distribution of women by body mass index according to background characteristics in Bangladesh
|
Characteristics |
Under weight |
Normal |
Overweight |
Obese |
|
Age |
|
|
|
|
|
15-19 |
28.38 |
64.13 |
6.19 |
1.31 |
|
20-24 |
21.01 |
62.05 |
14.67 |
2.27 |
|
25-29 |
16.34 |
59.99 |
20.31 |
3.37 |
|
30-34 |
13.32 |
55.79 |
25.11 |
5.78 |
|
35-39 |
13.61 |
56.36 |
23.51 |
6.53 |
|
40-44 |
17.71 |
54.13 |
21.92 |
6.23 |
|
45-49 |
19.85 |
53.33 |
21.09 |
5.73 |
|
Place of residence |
||||
|
Urban |
11.99 |
52.03 |
27.35 |
8.63 |
|
Rural |
20.62 |
60.76 |
15.98 |
2.64 |
|
Educational attainment |
||||
|
No education |
23.76 |
60.27 |
13.45 |
2.52 |
|
Primary |
20.08 |
59.45 |
16.77 |
3.7 |
|
Secondary |
15.16 |
57.47 |
22.12 |
5.26 |
|
Higher |
8.58 |
52.17 |
31.57 |
7.69 |
|
Source of drinking water |
||||
|
Piped water |
8.94 |
48.07 |
31.46 |
11.52 |
|
Tubewell/borewell |
18.98 |
59.4 |
18.03 |
3.6 |
|
Protected well |
30.84 |
50.08 |
19.08 |
0 |
|
Unprotected well |
24.57 |
73.32 |
2.12 |
0 |
|
River/dam/springs |
26.23 |
62.51 |
8.6 |
2.67 |
|
Others |
19.46 |
58.03 |
18.95 |
3.56 |
|
Type of fuel used for cooking |
||||
|
Clean |
7.93 |
48.61 |
32.38 |
11.08 |
|
Wood |
18.66 |
59.24 |
18.52 |
3.58 |
|
Crop residual |
22.55 |
62.25 |
13.29 |
1.91 |
|
Animal dung |
22.46 |
61.61 |
13.82 |
2.12 |
|
Others |
20.72 |
58.69 |
17.17 |
3.42 |
|
Current marital status |
||||
|
Never in union |
||||
|
Currently married |
17.67 |
58.47 |
19.52 |
4.35 |
|
Others |
26.94 |
55.42 |
13.67 |
3.98 |
|
Sex of household H |
||||
|
Male |
18.22 |
58.55 |
18.96 |
4.27 |
|
Female |
17.87 |
56.33 |
21.04 |
4.77 |
|
Type of toilet facilities |
||||
|
Flush toilet |
9.18 |
49.39 |
31.22 |
10.22 |
|
Pit laterine |
19.27 |
60.34 |
17.21 |
3.18 |
|
Open |
30.83 |
59.82 |
8.14 |
1.21 |
|
Other |
22.77 |
59.5 |
14.94 |
2.79 |
|
Wealth quintile |
||||
|
Poorest |
30.96 |
60.42 |
7.74 |
0.88 |
|
Poorer |
24.12 |
62.85 |
11.83 |
1.21 |
|
Middle |
18.58 |
61.69 |
17.04 |
2.7 |
|
Richer |
12.19 |
60.72 |
22.35 |
4.74 |
|
Richest |
7.02 |
46.65 |
34.98 |
11.35 |
|
Total |
18.18 |
58.3 |
19.19 |
4.33 |
Source: Demographic and Health Survey: Bangladesh- 2014
Children: According to the National Institute of Population Research and Training, undernutrition is a significant public health issue in Bangladesh (National Institute of Population Research and Training, 2009). Severe wasting is most common among children under one year old. Children from rural areas tend to have lower weight for their age (severely underweight: Z-score < -3.0 SD below the mean) compared to children living in urban areas. The majority of undernourished children come from poor households. Children of mothers with marital status of "others" (e.g., separated or divorced) are more likely to be undernourished compared to children of married women. Additionally, children of uneducated women are more likely to be moderately stunted or underweight. More than one-third of children with uneducated mothers are moderately underweight, accounting for approximately 33.04% of under-five children (Table 2). This leads to severe acute malnutrition, which significantly increases the chances of infection and hinders children's growth, ultimately affecting their physical and mental development (Ahmed et al., 2012).
Table 2: Percentage distribution of nutritional status of children according to background characteristics in Bangladesh
|
Characteristics |
Severe stunt |
Moderate stunt |
Severe waste |
Moderate waste |
Severe under weight |
Moderate under weight |
|
Age in months |
||||||
|
00-12 |
4.89 |
18.31 |
5.86 |
26.56 |
5.49 |
21.57 |
|
13-24 |
15.2 |
40.98 |
3.07 |
19.39 |
8 |
32.82 |
|
25-36 |
13.45 |
41.35 |
2.38 |
16.83 |
9.35 |
37.49 |
|
37-48 |
13.72 |
44.35 |
1.68 |
16.04 |
7.94 |
35.53 |
|
49-60 |
12.17 |
39.53 |
2.4 |
16.08 |
9.02 |
39.67 |
|
Place of residence |
||||||
|
Urban |
9.8 |
30.91 |
3.09 |
12.27 |
6.68 |
26.31 |
|
Rural |
12.47 |
38.45 |
3.17 |
15.47 |
8.29 |
35.31 |
|
Educational attainment mother |
||||||
|
No Education |
18.46 |
47.69 |
3 |
15.13 |
12.42 |
42.53 |
|
Primary |
15.36 |
44.18 |
3.53 |
15.83 |
10.31 |
39.5 |
|
Secondary |
8.79 |
31.4 |
2.95 |
14.18 |
5.92 |
28.81 |
|
Higher |
4.43 |
19.83 |
3.21 |
12.75 |
2.51 |
18.17 |
|
Source of drinking water |
||||||
|
Piped water |
11.61 |
31.11 |
3.3 |
14.53 |
9.14 |
23.81 |
|
Tubewell/borewell |
11.74 |
37.26 |
3.15 |
14.57 |
7.97 |
33.97 |
|
Protected well |
0 |
7.13 |
0 |
6.76 |
0 |
40.96 |
|
Unprotected well |
21.43 |
53.76 |
6.96 |
12 |
6 |
44.33 |
|
River/dam/springs |
15.72 |
41.84 |
6.85 |
22.13 |
15.53 |
41.63 |
|
Others |
11.61 |
34.18 |
2.31 |
14.77 |
5.19 |
31.42 |
|
Type of fuel used for cooking |
||||||
|
Clean |
8.48 |
26.52 |
3.35 |
11.33 |
6.06 |
20.35 |
|
Wood |
11.57 |
36.86 |
3.23 |
15.12 |
7.56 |
32.89 |
|
Crop residual |
12.95 |
41.9 |
3.11 |
15.1 |
9.29 |
40.37 |
|
Animal dung |
16.05 |
41.6 |
3.64 |
17.12 |
12.59 |
40.28 |
|
Others |
12.17 |
34.03 |
2.11 |
14.54 |
5.65 |
30.73 |
|
Current marital status of mother |
||||||
|
Never in union |
NA |
|||||
|
Currently married |
11.76 |
36.44 |
3.13 |
14.65 |
7.87 |
32.93 |
|
Others |
14.79 |
44.78 |
4.54 |
15.84 |
9.3 |
41.88 |
|
Sex of household H |
||||||
|
Male |
11.94 |
36.86 |
2.92 |
14.56 |
8.03 |
32.99 |
|
Female |
10.34 |
33.33 |
5.55 |
15.77 |
6.44 |
33.62 |
|
Type of toilet facilities |
||||||
|
Flush toilet |
7.86 |
23.48 |
2.14 |
12.53 |
6.19 |
19.97 |
|
Pit latrine |
11.79 |
38.58 |
3.46 |
14.86 |
7.95 |
34.82 |
|
Open |
21.34 |
43.12 |
6.07 |
21.25 |
15.21 |
44.8 |
|
Other |
14.81 |
40.49 |
2.04 |
14.85 |
8.09 |
37.31 |
|
Wealth quintile |
||||||
|
Poorest |
18.7 |
49.45 |
3.78 |
17.47 |
13.14 |
46.39 |
|
Poorer |
13.17 |
43.19 |
3.69 |
16.89 |
8.84 |
39.13 |
|
Middle |
11.87 |
36.59 |
2.76 |
13.21 |
7.39 |
32.28 |
|
Richer |
8.53 |
31.49 |
2.58 |
13.44 |
5.46 |
27.51 |
|
Richest |
5.45 |
19.58 |
2.85 |
11.86 |
3.69 |
17.44 |
|
Total |
11.8 |
36.55 |
3.15 |
14.66 |
7.89 |
33.04 |
Source: Demographic and Health Survey: Bangladesh- 2014
Determinants of Diet
The health indicator of anaemia among women and child denotes the necessity for more long-term interventions. We need to note that the dietary diversity within the country might affect health along with variable accessibility to interventions. Table 3 presents the percentage distribution of the diet of 'children under five years old. Only 1% of children in 49-60 months' age consumed Legume. The children residing in rural areas had a higher proportion of fruits as compared to urban children (Rural 18.9 % vs Urban 16.7). The children whose mothers had the highest education gave their children a higher proportion of flesh (17.7 vs 10.5) and dairy products (19.2 vs 13.8) as compared to children of illiterate mothers. The children from the richest wealth quintile ate more dairy and legumes than those from the poorest wealth quintile. Unexpectedly, the children from the richest wealth quintile household reported having a lesser proportion of dairy products whereas children from the poorest household consumed more (9.0 vs 13.6). This might occur due to poor awareness about a balanced diet among mothers. This must be one of the reasons for micronutrient deficiencies and Malnutrition. Also, the proportion of women providing exclusive breastfeeding seems to be questionable when under six months of children were given different foods. Undoubtedly, this leads to undernutrition and infant mortality.
Table 3: Percentage distribution diet of children with the age group in Bangladesh
|
Characteristics |
Grain |
Potato |
Legume |
Dairy |
Flesh |
Egg |
Fruit/veg |
|
Age in months |
|||||||
|
00-12 |
43.3 |
18.4 |
3.1 |
19.6 |
14.4 |
11.8 |
20.6 |
|
13-24 |
76.6 |
44.0 |
8.0 |
31.0 |
43.7 |
31.3 |
50.0 |
|
25-36 |
6.0 |
2.8 |
0.5 |
2.7 |
3.0 |
1.9 |
3.0 |
|
37-48 |
9.7 |
4.5 |
0.8 |
3.8 |
4.9 |
2.6 |
5.0 |
|
49-60 |
12.5 |
6.9 |
1.0 |
3.6 |
5.7 |
3.5 |
7.5 |
|
Place of residence |
|||||||
|
Urban |
30.9 |
15.6 |
3.5 |
13.0 |
14.3 |
11.9 |
16.7 |
|
Rural |
30.0 |
15.7 |
2.4 |
12.2 |
14.8 |
9.8 |
18.0 |
|
Educational attainment of mother |
|||||||
|
No education |
26.2 |
12.7 |
1.7 |
7.3 |
10.5 |
5.8 |
13.8 |
|
Primary |
29.2 |
14.4 |
2.4 |
10.4 |
13.9 |
8.2 |
16.2 |
|
Secondary |
32.1 |
17.4 |
3.4 |
14.5 |
15.9 |
12.2 |
19.3 |
|
Higher |
31.2 |
15.6 |
2.1 |
16.7 |
17.7 |
16.1 |
19.2 |
|
Sex of household Head |
|||||||
|
Male |
30.3 |
15.7 |
2.7 |
12.6 |
14.7 |
10.4 |
17.4 |
|
Female |
30.1 |
14.5 |
3.2 |
11.3 |
13.8 |
10.6 |
19.2 |
|
Type of toilet facilities |
|||||||
|
Flush toilet |
29.7 |
13.4 |
3.9 |
13.6 |
13.0 |
12.6 |
16.0 |
|
Pit laterine |
30.4 |
16.4 |
2.4 |
12.1 |
15.1 |
10.1 |
18.0 |
|
Open |
25.3 |
12.4 |
1.0 |
14.4 |
8.2 |
8.2 |
14.9 |
|
Other |
31.1 |
14.7 |
3.3 |
12.5 |
15.8 |
10.3 |
17.9 |
|
Wealth quintile |
|||||||
|
Poorest |
31.6 |
16.5 |
2.0 |
9.0 |
13.7 |
8.1 |
17.7 |
|
Poorer |
27.8 |
15.2 |
2.1 |
10.8 |
13.6 |
8.5 |
18.0 |
|
Middle |
30.3 |
16.2 |
2.2 |
13.9 |
15.5 |
9.2 |
17.9 |
|
Richer |
31.6 |
16.1 |
3.7 |
15.4 |
16.5 |
12.4 |
17.2 |
|
Richest |
29.8 |
14.1 |
3.6 |
13.6 |
13.9 |
14.2 |
16.9 |
|
Total |
30.3 |
15.6 |
2.7 |
12.5 |
14.6 |
10.5 |
17.6 |
Source: Demographic and Health Survey: Bangladesh- 2014
Determinant of nutritional status
The table 4 shows, the determinant of women's education had strong significance with underweight women. Looking at the differentials of education, the formally educated women were 2.11 times more likely to be obese (OR 2.11 at 95% CI [1.64-2.7]) than illiterate women. It was statistically significant (p < .001). Further, we calculated associations for other variables, we found that the women residing in rural areas were 1.03 times more likely to become underweight than those from urban regions and it was significantly associated (OR1.03at 95% CI [0.92-1.16]). The women in the menopausal age group of 40-44yrs were 8.11 times more likely to be obese than 15-19yrs women (OR 8.11 95%CI [5.12-12.62]). When we used the regression model, BMI by cooking fuel, we measured that the women who were living in households having kitchens with wood as fuel for cooking were 1.19 times more likely to be underweight than those having a supply of clean fuel (1.19 at 95% CI [0.98-1.46]). Then, while associating BMI by wealth index, the women who lived in the richest houses were 8.44 times more likely to be obese (BMI>=30.0 kg/m2) than women who lived in the poorest houses and significantly associated (8.44 95%CI [5.26-13.54]). Therefore, the wealth index is a significant indicator of economic status which has an impact on the nutritional status.
Table 4: Results of binary logistic odds ratio of Under-weight, Overweight and Obese females 15-49years in Bangladesh
|
Characteristics |
Under-weight |
Overweight |
Obese |
|
Age of mothers |
|||
|
15-19 ® |
|
|
|
|
20-24 |
0.75***(0.66,0.86) |
2.46***(1.99,3.05) |
1.75**(1.11,2.76) |
|
25-29 |
0.55***(0.48,0.63) |
3.84***(3.12,4.73) |
3.03***(1.96,4.69) |
|
30-34 |
0.45***(0.39,0.53) |
5.65***(4.58,6.96) |
6.29***(4.11,9.62) |
|
35-39 |
0.43***(0.37,0.52) |
5.65***(4.54,7.03) |
7.58***(4.91,11.7) |
|
40-44 |
0.57***(0.48,0.68) |
5.79***(4.62,7.25) |
8.11***(5.21,12.62) |
|
45-49 |
0.65***(0.54,0.77) |
5.74***(4.55,7.24) |
7.5***(4.76,11.83) |
|
Place of residence |
|||
|
Urban ® |
|
|
|
|
Rural |
1.03(0.92,1.16) |
0.85***(0.77,0.95) |
0.64***(0.53,0.78) |
|
Sex of household H |
|||
|
Male ® |
|
|
|
|
Female |
0.96(0.83,1.11) |
1.13*(0.99,1.29) |
1.07(0.83,1.36) |
|
Source of drinking water |
|||
|
Piped water ® |
|
|
|
|
Tubewell /borewell |
0.93(0.74,1.15) |
0.99(0.85,1.15) |
0.9(0.72,1.14) |
|
Protected well |
1.56(0.7,3.51) |
1.49(0.57,3.91) |
0 |
|
Unprotected well |
0.66(0.39,1.12) |
0.18**(0.05,0.74) |
0 |
|
River/dam/springs |
0.88(0.6,1.3) |
0.7(0.42,1.16) |
1.41(0.58,3.42) |
|
Others |
0.8(0.53,1.2) |
1.35*(0.95,1.93) |
0.75(0.38,1.48) |
|
Type of fuel used for cooking |
|||
|
Clean ® |
|
|
|
|
Wood |
1.19*(0.98,1.46) |
0.87**(0.75,1) |
0.75**(0.59,0.95) |
|
Crop residual |
1.03(0.82,1.28) |
0.89(0.75,1.06) |
0.75*(0.54,1.05) |
|
Animal dung |
1.11(0.87,1.43) |
0.88(0.7,1.1) |
0.76(0.47,1.22) |
|
Others |
1.32(0.89,1.97) |
0.79(0.53,1.18) |
0.92(0.43,1.96) |
|
Type of toilet Facilities |
|||
|
Flush toilet ® |
|
|
|
|
Pit laterine |
0.89(0.75,1.06) |
1.02(0.9,1.16) |
0.94(0.76,1.16) |
|
Open |
0.95(0.73,1.23) |
1.08(0.76,1.52) |
1.36(0.6,3.1) |
|
Other |
0.91(0.7,1.19) |
0.99(0.72,1.37) |
1.26(0.63,2.49) |
|
Current marital status |
|||
|
Never in union ® |
|
|
|
|
Currently married |
|||
|
Others |
1.57***(1.32,1.87) |
0.64***(0.52,0.79) |
0.72*(0.5,1.04) |
|
Educational attainment |
|||
|
No education ® |
|
|
|
|
Primary |
0.86***(0.77,0.95) |
1.33***(1.18,1.51) |
1.62***(1.26,2.07) |
|
Secondary |
0.73***(0.64,0.83) |
1.73***(1.52,1.96) |
2.11***(1.64,2.7) |
|
Higher |
0.6***(0.48,0.75) |
1.81***(1.53,2.15) |
1.73***(1.27,2.36) |
|
Wealth quintile |
|||
|
Poorest ® |
|
|
|
|
Poorer |
0.76***(0.67,0.85) |
1.34***(1.12,1.6) |
1.24(0.75,2.03) |
|
Middle |
0.61***(0.54,0.69) |
1.82***(1.53,2.16) |
2.57***(1.64,4.04) |
|
Richer |
0.4***(0.35,0.47) |
2.31***(1.94,2.75) |
4.03***(2.58,6.29) |
|
Richest |
0.32***(0.26,0.4) |
3.89***(3.18,4.76) |
8.44***(5.26,13.54) |
Note:CI-95%, Significance ***p < .001., ** p <0.01, *p < 0.05 , ® Reference category
Table 5, the variables of nutrition were compared with the household factors, factors about the mother such as age, marital and educational status. The children from the poorer households were 0.81 times more likely to be moderately underweight than children from the poorest households (0.81 at 5%CI [0/81-0.81]). The children whose mothers had attainment of primary education were 1.25 times higher likelihood to suffer from severe wasting than children of Illiterate mothers. The likelihood of children from rural areas is 1.17 more than urban areas to have moderate wasting. Compared to children having a house with clean piped water, severe wasting was 1.62 times more likely among children drinking water from unprotected wells. And the likelihood of children defecating in open was 2.95 times higher for severe wasting than children having a flush toilet. The data shows significant wasting among children who were defecating in open spaces. There were activities by the government to reduce open defecation in the mid-2000s. However, the data shows still a lack of access to potable water and proper sanitation. Studies have shown a positive association between a mother's and child's health (Saha, et al., 2019). The present study reiterates these findings and highlights the consequences of contaminated water and poor sanitation in rural areas.
Table 5: Results of binary logistic odds ratio of stunting, wasting and underweight among children age 0-59 months in Bangladesh
|
Characteristics |
Severe stunt |
Moderate stunt |
Severe waste |
Moderate waste |
Severe under weight |
Moderate under weight |
|
|
Wealth quintile |
|||||||
|
Poorest ® |
|
|
|
|
|
|
|
|
Poorer |
0.72*** |
0.82*** |
0.95*** |
0.96*** |
0.72*** |
0.81*** |
|
|
Middle |
0.7*** |
0.67*** |
0.7*** |
0.72*** |
0.63*** |
0.65*** |
|
|
Richer |
0.42*** |
0.51*** |
0.62*** |
0.76*** |
0.36*** |
0.53*** |
|
|
Richest |
0.21*** |
0.26*** |
0.72*** |
0.67*** |
0.16*** |
0.33*** |
|
|
Age of mothers |
|||||||
|
15-19 ® |
|
|
|
|
|
|
|
|
20-24 |
1.47*** |
1.13*** |
0.71*** |
0.81*** |
1.11*** |
1.11*** |
|
|
25-29 |
1.3*** |
1.19*** |
0.77*** |
0.71*** |
0.93*** |
1.06*** |
|
|
30-34 |
1.38*** |
1.11*** |
0.54*** |
0.83*** |
1.16*** |
1.14*** |
|
|
35-39 |
1.19*** |
1.13*** |
0.86*** |
0.75*** |
0.84*** |
1.07*** |
|
|
40-44 |
0.95*** |
1.19*** |
0.13*** |
0.38*** |
0.67*** |
0.79*** |
|
|
45-49 |
5.73*** |
3.36*** |
3.84*** |
0.9*** |
2.53*** |
2.46*** |
|
|
Place of residence |
|||||||
|
Urban ® |
|
|
|
|
|
|
|
|
Rural |
0.91*** |
0.91*** |
0.91*** |
1.17*** |
0.93*** |
0.93*** |
|
|
Sex of household H |
|||||||
|
Male ® |
|
|
|
|
|
|
|
|
Female |
0.9*** |
0.9*** |
2*** |
1.11*** |
0.84*** |
1.1*** |
|
|
Source of drinking water |
|||||||
|
Piped water ® |
|
|
|
|
|
|
|
|
Tubewell/borewell |
0.48*** |
0.61*** |
0.87*** |
0.6*** |
0.38*** |
0.72*** |
|
|
Protected well |
1*** |
0.07*** |
1*** |
0.24*** |
1***(0, |
0.95*** |
|
|
Unprotected well |
0.71*** |
0.95*** |
1.62*** |
0.37*** |
0.2***( |
0.84*** |
|
|
River/dam/springs |
0.41*** |
0.5*** |
1.6*** |
0.82*** |
0.53*** |
0.7*** |
|
|
Others |
0.45*** |
0.71*** |
1.5*** |
0.78*** |
0.26*** |
1.02*** |
|
|
Type of fuel used for cooking |
|||||||
|
Clean ® |
|
|
|
|
|
|
|
|
Wood |
0.91*** |
0.94*** |
0.67*** |
1.42*** |
0.92*** |
1.19*** |
|
|
Crop residual |
0.71*** |
0.81*** |
0.59*** |
1.28*** |
0.8*** |
1.21*** |
|
|
Animal dung |
1*** |
0.85*** |
0.71*** |
1.52*** |
1.24*** |
1.29*** |
|
|
Others |
0.85*** |
0.55*** |
0.4*** |
1.15*** |
0.87*** |
0.61*** |
|
|
Type of toilet Facilities |
|||||||
|
Flush toilet ® |
|
|
|
|
|
|
|
|
Pit laterine |
0.86*** |
1.19*** |
2.06*** |
0.94*** |
0.64*** |
1.14*** |
|
|
Open |
1.14*** |
0.98*** |
2.95*** |
1.24*** |
0.83*** |
1.18*** |
|
|
Other |
1.16*** |
1.61*** |
1.13*** |
0.86*** |
0.77*** |
1.53*** |
|
|
Current marital status of mother |
|||||||
|
Never in union ® |
|
|
|
|
|
|
|
|
Currently married |
1*** |
1.26*** |
0.91*** |
0.96*** |
0.93*** |
1.21*** |
|
|
Educational attainment of mother |
|||||||
|
No education ® |
|
|
|
|
|
|
|
|
Primary |
0.88*** |
0.94*** |
1.25*** |
1.06*** |
0.9*** |
0.97*** |
|
|
Secondary |
0.59*** |
0.7*** |
1.18*** |
1.03*** |
0.65*** |
0.76*** |
|
|
Higher |
0.36*** |
0.5*** |
1.41*** |
1.05*** |
0.34*** |
0.56*** |
|
Note: CI-95%, Significance ***p < .001. ** p <0.01, *p < 0.05 , ® Reference category
Discussion and Analysis
The government's participation in several international conferences, including the first International Conference on Nutrition was held in 1992 and the World Food Summit of 1996, made it aware of the significance of nutrition as an issue for national development (Gillespie et al., 2013). Bio-psycho-social risk factors can contribute to poor nutrition in children. Despite these multiple risk factors, interdisciplinary collaboration between experts in psycho-social dimensions and those in the biological aspects of nutrition has not been commonly practiced. In Israel, an evaluation was conducted to assess the collaboration between social workers and dieticians in leading nutrition-education programs, which finds more successful (Shor R., 2010). The National Food Security and Nutrition Policy of 1997, the government role in the International Conference on Nutrition played the most crucial role (Shahan, A. M., & Jahan, F. (2017). The National Food and Nutrition Policy (NFNP) of 1997 for the first time identified undernutrition as a major developmental problem and according to the policy document: "Malnutrition is endemic in the country, with the high infant, under-five and maternal morbidity and mortality. About 94 % of the children are malnourished and 30,000 are becoming blind from vitamin A deficiency every year. Almost the whole population suffers from micronutrient deficiencies such as iodine, iron, zinc, vitamin A, and riboflavin" (Shahan, A. M., & Jahan, F. (2017). The Bangladesh Integrated Nutrition program was implemented in 1997, it involved a community-based approach to combat Malnutrition. Also mentor's role and qualities were crucial in enhancing the impact of the interventions. Mentoring circles present a promising strategy for workforce development in the fields of nutrition and dietetics (Georgia D. et.al., 2023).
In 2018, Food and agriculture organizations had reported 15.2 % of the total population is undernourished in Bangladesh. Also, it was studied to have poor diet diversity and comprises mostly fish, some vegetables, rice (FAO (Food and agriculture organization of United Nations, 2016). The results of this study explain probable causes of Malnutrition and anaemia found in this study findings. While Bangladesh has seen impressive reductions in poverty, it is still a significant factor influencing Malnutrition: 54 % of children in the lowest wealth quintile are stunted compared to 26 % in the highest (Chaparro, Oot, & Sethuraman, 2014; Hossain et al.,2005).
A national nutrition survey on food intake in the Bangladeshi population, found a declining trend in nutrient intake, has been assessed. Following this, Bangladesh National Nutrition Council (BNNC) prepared the Nutrition Policy and Program for Bangladesh, which was approved by the BNNC and published in 1984, and the government adopted National Food Policy 2006 (Mannan, 2003; Islam, M. Z., Riaz, L., et al., 2018). BNNC gave the dietary guidelines for various age groups. The government allocation of budget is raised in its contribution of almost 7% for three sectors of health, nutrition, and population (Nisbett, Davis, Sivan Yosef, & Nazneen Akhtar, 2017). Bangladesh shows slow and steady improvement in the parameter of anaemia. Social inequity prevails predominant reason for poor nutritional indicators. In 2014 Ministry of Finance, Bangladesh noted the major challenge during the country's economic progress was rural-urban disparity.
The graphical representation of the prevalence of anaemia (Figure 1) reflects the changes over these years influenced due to various government activities such as deworming, micronutrient supplementation, growth monitoring. Thus, the political will to collaborate during the nutrition policy implementation gets reinstated as the various stakeholders should come together to handle this issue (Shahan, A. M., & Jahan, F. (2017). The poorest and uneducated women and their children seem to have a tough time fulfilling their recommended nutritional intake. The present study supports the prevalence of anaemia due to the rich-poor gap. Bangladesh has a predominantly patriarchal society which causes gender discrimination during the distribution of foods at the household level. Also, the choice of foods depends on the cost for procurement and so expensive but nutritious foods such as milk, fish, fruits are less consumed. This gets reflected in analysis of the dietary intake of children. It showed inadequate nutritional intake of fruits and vegetables. However, the country is facing a double burden of issues in form of undernutrition and the impending obesity issue. This resonates with this study's findings.
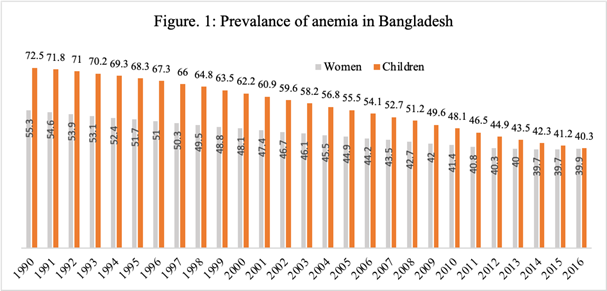
Source: World Health Organization, Global Health Observatory Data Repository/World Health Statistics (apps.who.int/gho/data/node.main.1?lang=en ).(27/09/2020, 11.am)
Implications for Health Social Work Practice
Clinical and medical social work practice has been a dominant force in the social work discipline since its inception. The diagnostic social work intervention has significantly contributed to the development of medical social work settings in both developing and developed countries. Health is a core domain of social work education and practice, encompassing public health, community health, and mental health. Globally, many social work institutions offer degrees in Public and Mental Health specialization. During the COVID-19 pandemic, health social workers highlighted long-standing health disparities among patient populations, necessitating adaptations in their work. It is argued that social work is in a prime position to lead efforts toward more equitable health outcomes. Rising inequitable health access services contribute to deprivation, vulnerability, and malnutrition among marginalized social groups, with serious implications for their well-being. In Bangladesh, there is a free universal health care system, but it is characterized by a shortage of doctors, nurses, medicine, and medical equipment, particularly in rural areas. Over the last two decades, private medical care services have boomed, mainly in urban areas, making it unaffordable for the rural poor due to inadequate income. Social work educators, practitioners, policy researchers, and civil society organizations need to address these concerns. Social workers in the health sector in Bangladesh also need a technical and empirical understanding of nutritional aspects before conceptualizing social work or policy interventions. They are not only involved at the individual level, but also concerned with policy-level macro interventions for the overall well-being of women and children in the state. Social workers' solidarity is crucial in influencing policy to make the state more accountable and welfare-friendly. The discussion and analysis take into account various socio-economic, gender, and cultural aspects that can help health social workers understand the complexity when proposing research or social work interventions.
Conclusion
The DHS data is used in this paper to highlight the increasing concern of the double burden of malnutrition in Bangladesh, where the prevalence of overweight among women is greater than underweight. Women's and children's nutrition remains a significant issue in the country, with the government recognizing the need to address both undernutrition and the growing risk of overweight/obesity among women. Bangladesh also faces a growing problem of obesity alongside undernourished children. Wasting, an acute form of malnutrition, can be addressed more rapidly with adequate food supply and safety nets for food security. The poor nutritional health indicators among underprivileged women and children emphasize the need for long-term interventions. Factors such as wealth index, access to education, and place of residence continue to negatively affect the health status of women and children. There have been improvements in agricultural production and financial allocation to tackle these issues. Research is needed to identify the social and cultural factors that influence community-specific interventions. Health social work practitioners can play vital roles by implementing strategic and innovative interventions for social mobilization, leading policy advocacy campaigns to secure political commitment to reduce poverty, and effecting positive change in the community. They can also work to improve educational awareness and advocate for policies to enhance the implementation of health programs. Finally, a strong support system that prioritizes a multi-sectoral approach for nutrition will coordinate the successful implementation of nutritional policies through a national-level network involving civil society, academia, policy researchers, and government active involvement.
Strengths and Limitations of the study
The study provides nationally representative measures of nutritional parameters for children under the age of five and women of reproductive age in Bangladesh. The wealth index is a variable calculated during the survey. We acknowledge that it might not accurately reflect current economic status. However, the different assets considered for the measurement of the Wealth Index provide representative information. It's important to note that dietary diversity within the country might affect health, along with variable accessibility to interventions. The study does not capture unobserved regional variations within the state, but the national level measures are still a valuable contribution. Further research is needed to gain rich and in-depth insights and experiences from various stakeholders, service providers, and beneficiaries involved in nutrition policies.
Declarations:
Ethics approval and consent to participate.
Not applicable
Consent for publication.
Not applicable
Availability of data and materials
Data has been taken from the Global Health Observatory Data Repository (GHODR), Demographic Health Survey (DHS) and reviews some of the critical interventions in nutrition within the different countries and draws out several issues that bear on these policies' future evolution which are publicly available.
Conflict of Interest
No conflict of interest was reported by all authors.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgements
This study would not have been possible without the enthusiastic cooperation as well as the advice of our respected professor R.B. Bhagat.
References:
Adams, A. M., Mridha, M. K., et al. (2014). Maternal Undernutrition and Excessive Body Weight and Risk of Birth and Health Outcomes. Archives of Public Health, 72(1), 4.
Ahmed, S. M., Adams, A., Chowdhury, A. M. R., & Bhuiya, A. (1998). Chronic Energy Deficiency in Women from Rural Bangladesh: Some Socioeconomic Determinants. Journal of Biosocial Science, 30(3), 349–358. doi:10.1017/S0021932098003496
Ahmed, T., Mahfuz, M., Ireen, S., Ahmed, A. S., Rahman, S., Islam, M. M., Cravioto, A. (2012). Nutrition of Children and Women in Bangladesh: Trends and Directions for the Future. Journal of Health, Population and Nutrition, 1-11.
Arnold, F., Nangia, P., & Kapil, U. (2004). Indicators of Nutrition for Women and Children: Current Status and Recommendations. Economic and Political Weekly, 664-670.
Ashcroft, R., Lam, S., Kourgiantakis, T., Begun, S., Nelson, M., Adamson, K., Cadell, S., Walsh, B., Greenblatt, A., Hussain, A., Sur, D., Sirotich, F., & Craig, S. L. (2021). Preparing social workers to address health inequities emerging during the COVID-19 pandemic by building capacity for health policy: A scoping review protocol. BMJ Open, 11(11), 1–7. https://doi.org/10.1136/bmjo pen-2021-053959
Barbara Berkman (1996) The Emerging Health Care World: Implications for Social Work Practice and Education, Social Work, Volume 41, Issue 5, 541–551, https://doi.org/10.1093/sw/41.5.541
Chaparro, C., Oot, L., & Sethuraman, K. (2014). Bangladesh Nutrition Profile. Washington, DC: FHI 360/FANTA.
Craig, S. L., Kourgiantakis, T., Kirkland, A., Muskat, B., & Sur, D. (2022). Riding the wave: Pandemic social work in hospitals. Social Work in Health Care, 61(5), 323–337. https://doi.org/10.1080/00981389.2022.2085232
Findley P. A. (2020). Health and nutrition: Social work's role. Social work in health care, 59(7), 513–524. https://doi.org/10.1080/00981389.2020.1804035
Gautham, P., Nazneen, S., et al. (2015). Child Malnutrition in Bangladesh: Evidence from a Literature Review. Asia Pacific Journal of Public Health, 27(2), NP2386-NP2398.
Georgia Day, Jorja Collins, Cliona Twohig, Khia De Silva, Julie Brimblecombe, (2023).Towards healthy food retail: An assessment of public health nutrition workforce capacity to work with stores, Australian and New Zealand Journal of Public Health, Volume 47, Issue 3, 100056, ISSN 1326-0200, https://doi.org/10.1016/j.anzjph.2023.100056.
Gillespie, S., Haddad, L., Mannar, V., Menon, P., & Nisbett, N. (2013). The politics of reducing Malnutrition: building commitment and accelerating progress. The lancet, 382(9891), 552-569
Global Nutrition Report (2020): Action on equity to end Malnutrition. Bristol, UK: Development Initiatives.
Hossain, M. A., Ahmed, F., et al. (2014). Determinants of Chronic Malnutrition among Preschool Children in Bangladesh. Journal of Biosocial Science, 46(3), 425-439.
Hossain, M., Naher, F., & Shahabuddin, Q. (2005). Food security and nutrition in Bangladesh: progress and determinants. EJADE: Electronic Journal of Agricultural and Development Economics, 2(853-2016-56126), 103-132.
Hossain, I., Alam, M. J., & Islam, M. N. (2005). Medical social work practices for the improvement of health care system in Bangladesh. Journal of Sociology, 1(1), 63–74
Hossain, I and Mathbor, M.G (2014) Social Work Practice for Social Development in Bangladesh: Issues and Challenges, Asian Social Work and Policy Review 8, 123–137 https://doi.org/10.1111/aswp.12030
Islam, M. Z., Riaz, L., et al. (2018). Nutritional Status of Children in Bangladesh: Measuring Composite Index of Anthropometric Failure (CIAF) and its Determinants. PLOS ONE, 13(11), e0206926.
Magnani, R., Oot, L., Sethuraman, K., Kabir, G., & Rahman, S. (2015). USAID Office of Food for Peace Food Security Country Framework for Bangladesh FY 2015–2019. Washington, DC: FHI 360/FANTA.
Mannan, M. A. (2003). An evaluation of the national food and nutrition policy of Bangladesh. Food and Nutrition Bulletin, 183-192.
National Institute of Population Research and Training - NIPORT/Bangladesh, Mitra and Associates/Bangladesh, and Macro International (2009). Bangladesh Demographic and Health Survey 2007. Dhaka, Bangladesh: NIPORT, Mitra and Associates, and Macro International. Available at http://dhsprogram.com/pubs/pdf/FR207/FR207.pdf.
Nisbett, N., Davis, P., Sivan Yosef, & Nazneen Akhtar. (2017). Bangladesh's story of change in nutrition: Strong improvements in basic and underlying determinants with an unfinished agenda for direct community level support. Global Food Security, Volume 13, 21-29.
Raihan, M. J., Shamim, A. A., et al. (2017). Bangladesh National Nutrition Services: Assessment of Implementation Status. PLOS ONE, 12(7), e0170895.
Saha, Chattapadhay A and Richardus (2019) Trends, prevalence and determinants of childhood chronic under nutrition in regional divisions of Bangladesh: Evidence from demographic health surveys, 2011and2014.PLoS ONE14(8):e0220062.
Shahan, A. M., & Jahan, F. (2017). Opening the policy space: the dynamics of nutrition policy making in Bangladesh. Dhaka: Montpellier, France: Agropolis International, Global Support Facility for the National Information Platforms for Nutrition initiative.
Shor R. (2010). Interdisciplinary collaboration between social workers and dieticians in nutrition education programs for children-at-risk. Social work in health care, 49(4), 345–361. https://doi.org/10.1080/00981380903364775.
Tharakan, K. R. & Suchindran, P. S. (1999) Assessing potential risk factors for child malnutrition in rural Kerala, Botswana. Journal of Tropical Pediatrics 47, 350–355
Author´s Address:
Dr. Hanumant Waghmare
Department of Sociology and Social Work, Hemvati Nandan Bahuguna Garhwal
University
A Central University Srinagar, Uttarakhand
9867448516
hanumantw@gmail.com
Author´s Address:
Dr. Sudhir Maske
Department of Social Work, Delhi University, New Delhi
sudhir.dssw@gmail.com
Author´s Address:
Dr. Pooja Gaigaware
Tata Institute of Social Sciences, Mumbai
drpoojagaware@gmail.com