Domestic Violence, Mental Health, and COVID-19: A Community-based Study of Women in Delhi
Ajit Kumar Lenka, Noida International University
Neha Sharawat, Banasthali Vidyapith
Smritima Diksha Lama, Hitotsubashi University
Sanghmitra S Acharya, Jawaharlal Nehru University
Abstract: Domestic violence is a product of unequal gender power relations in the household. During the COVID-19 pandemic, due to restricted physical movement there was an increased risk of violence which further exacerbated the vulnerability of those already in abusive relationships. Several factors led to an increase in the number of domestic violence cases including loss of livelihoods, restriction of social contact within informal and informal networks, and limited access to services and community support. During the COVID-19 in many countries, data indicates an increase in reports of domestic violence, sexual harassment, and other forms of violence against women. The current paper is based on an empirical study using qualitative methods of data collection, conducted in Munirka urban village, Delhi. The paper focuses on the factors affecting the rate of increase in domestic violence cases during the COVID-19 pandemic, and subsequent effects on the mental health of women. Main finding of the study indicates that cases of domestic violence during COVID-19 increased due to alcoholism, loss of livelihood, financial insecurity, and limited access to services. Hence, authors suggest that to reduce the prevalence of violence against women, there should be an improvement in female education, raising awareness about their rights, and providing better social support.
Keywords: COVID-19, Domestic violence; Gender-based violence; Mental health; Slums; South Delhi; Alcoholism
Introduction
Violence against women is said to be a universal phenomenon experienced irrespective of country or context and is often considered a norm that is well-accepted (Srivastava et al., 2014). There is a plethora of literature that documents the relationship between alcoholism, domestic violence and their interplay that impacts upon an individuals’ mental health and wellbeing. It has been acknowledged that women disproportionately bear the health and psychological burdens of violence and domestic violence most often occurs in a safe space i.e. their homes and the perpetrator is usually a person they trust (Golder, 2016).
According to the global estimates, the prevalence of domestic violence, also called Intimate Partner Violence (IPV) is highest in South-East Asia i.e. 37.7% in comparison to other WHO regions. In India, the crime against women is rising and National Crime Records Bureau (NCRB), reported it as 64.5 % in 2021 compared to 56.3 % in 2014, while the highest crime rate of 147.6% was reported in the Union Territory of Delhi. Recognising the multi-dimensional and complex nature of IPV, the WHO recommends an ecological framework for violence prevention wherein several factors are said to influence violent behaviour separately and cumulatively at the individual, relationship, community, and societal levels (Wilson et al., 2014). Another study indicates that women with partners having alcohol problems were more likely to experience victimization, injury, mood disorders, anxiety disorders, and being in fair or poor health than women whose partners did not have alcohol problems. In addition, they were also said to experience more life stressors with lower mental/psychological quality of life scores (Dawson et al., 2007).
Existing literature in anthropology and sociology also highlights that structural violence is an important contributory factor that leads to domestic violence (Ghosh, 2015). Scheper-Hughes and Bourgois (2004) have pointed out that the violence of poverty, hunger, social exclusion and humiliation also inevitably translates into intimate and domestic violence. Thus, the social and cultural dimensions of violence are what give violence its power and meaning. There are many underlying causal factors attributed to domestic violence, such as the failure to perform household duties and responsibilities (Raj et al., 2010), economic stress, hierarchical gender relations (Visaria, 1999), illiteracy, belonging to lower caste (Yasmin et al., 2022), not having a male child (Sinha et al., 2012), other associated factors are the age at marriage, the number of living children, women's employment, and dowry.
Since 1983, domestic violence has been recognized as a criminal offence under Indian Penal Code (IPC) 498-A but it was as late as 2005 that with the enactment of the Protection of Women from Domestic Violence Act 2005 (PWDVA) that civil protections were provided to the victims of domestic violence. The Act that came into effect in 2006, gave a comprehensive definition of domestic violence and stated that all forms of physical, emotional, verbal, sexual and economic violence, and covers both actual acts of such violence and threats of violence. PWDVA also recognises marital rape and unlawful dowry demands and harassment of any form under this heading. The Act is primarily meant to provide protection from domestic violence for wives, live-in partners at the hands of husbands and male live-in partners or their kin members. It also provides protection to other women living in a household, such as widows, mothers, sisters. Despite such an Act in place violence against women and girls continues and is a challenge that needs to be addressed, more so in a patriarchal society like India. Any form of violence against women not only affects women’s physical and mental health but it also has an indirect detrimental effect on her natal family and her children. Besides, there is also the direct and indirect cost of violence against women and it is a significant public health issue. Such violence affects the capacity and ability of the vulnerable population to access civil, political and socio-economic rights.
Due to strict patriarchal norms (Kalokhe et al., 2017) domestic violence is rampant in India as there are strict gender roles, societal acceptance of wife beating, gender inequities, and a strong preference for male offspring, among other factors (Bhandari & Hughes, 2017). According to the NFHS-5 (2019-2021) fact sheet, the rate of violence among married women in the age range of 18-49 years has increased in 5 states. In Karnataka, it has doubled, from 21% to 44% of which more than one-third face spousal violence. The remaining 4 states are Bihar (40%), Manipur (40%), and Telangana (37%). In comparison, the top five states with the highest percentage of spousal violence were Manipur (55%), Telangana (46%) and the three remaining states i.e., Andhra Pradesh, Bihar, and Tamil Nadu 45 % of women (aged 15-49 years) had experienced spousal violence (physical/emotional/sexual). As a result, it is critical to recognise the interdependencies involved in intimate relationships, which are exacerbated by poverty, stigma, co-dependency, child abuse and neglect, poor mental health, and fear of police and social services intervention (Gadd et al., 2019).
The National Crime Records Bureau (NCRB) annual report (2021-2022) indicates a surge of 4% in crimes against women in India throughout 2022, including cases of cruelty by husbands and relatives, abductions, assaults, and rapes. The NCRB report details a substantial escalation in reported crimes against women (IPC+SLL) increasing from 3,71,503 cases in 2020 to 4,45,256 cases in 2022. The report highlighted that a significant proportion of crimes against women under the Indian Penal Code (IPC) involved 'Cruelty by Husband or His Relatives' (31.4%), 'Kidnapping and Abduction of Women' (19.2%), 'Assault on Women with Intent to Outrage her Modesty' (18.7%), and 'Rape' (7.1%). In the NCW annual report (2008-2016) as per complaints registered under different categories Delhi is one of the top ten states in India with the highest number of reported complaints and these numbers have only increased over the years with the exception of 2022-23.
Table 1 Top five states on complaints received by NCW between 2018-2023
|
State |
2018-2019 |
2019-2020 |
2020-2021 |
2021-2022 |
2022-2023 |
|
Uttar Pradesh |
11287 |
11636 |
13058 |
15445 |
17048 |
|
Delhi |
1733 |
1957 |
2971 |
3361 |
2822 |
|
Haryana |
1181 |
1171 |
1431 |
1460 |
1360 |
|
Bihar |
754 |
815 |
1402 |
1450 |
1336 |
|
Rajasthan |
733 |
768 |
1242 |
1117* |
1291 |
Source: Annual Report, 2018-2023, NCW; *Haryana (1396 & 1291) was amongst top ten and replaced Rajasthan at 5th rank in 2021-22 & 2022-23
Violence against women has also been conceptualized as an issue relating to the exertion of power and social control over women, and this forms the background for understanding various forms of violence as a continuum from sexual harassment to homicide (Pandey & Nath, 2014). Post Covid, the literature also elaborates on the impact of the pandemic on domestic violence with most indicating an increase in the instances of domestic violence against partners (Piquero et al., 2021). It was noted that during periods of crisis, there has been an increase in the rates of intimate partner violence, child, and elderly abuse, as a consequence of economic instability and stressful environments (Jones and Isham, 2020; Kourti et al, 2023). Covid not only impacted the health of the population but also caused large scale loss of lives and livelihoods while impacting economies of the world. Studies have also indicated an increase in mental health concerns related to the lockdown (Sedri et al., 2020).
Domestic violence was said to have been one of the major issues faced by women during the time of COVID-19. As per Vora et al. (2020) the violence against women increased after the state-wide lockdown was implemented in early April 2020. Specifically, in India there was an increase of 32% of domestic violence cases with most referring to intimate partner violence (Kourti et al, 2023). However, it is also important to highlight that there is systematic research suggesting that most instances of domestic violence against women remain unreported or underreported (Su et al., 2021).
Conceptual Framework
WHO (2024) outlined several factors influencing instances of intimate partner violence and sexual violence including at individual, family, community and wider society levels interacting with each other to increase or reduce risk of abuse. Some of the risk factors include low education levels, harmful use of alcohol, harmful masculine behaviour, community norms defining the status of women vs men, lack of access to women for paid employment, history of exposure to violence, marital discord, etc. It is critical to recognize that mental health issues manifest in various visible behavioral actions. Any stress or stimulant (job insecurity, poverty, lack of sleep, any other insecurity, dissatisfaction,) that causes an imbalance in the mental health begins to manifest in visible behavioral action, which may lead to the individual (or population) engaging in unethical behavior. The cyclic intersection of alcohol use, domestic violence and mental health rest on the vital role of institutional mechanisms, social support systems, and individual, familial and societal willingness to address the issues pertaining to this interstation of trajectories have been examined in this study.
In this context, considering that violence against women may be an issue relating to the exertion of power and social control, the paper has attempted to examine the conditions of women having poor socio-economic background resulting in them having fewer avenues in responding to problems associated with their lived experiences as victims of domestic violence. The paper explores the mental health problems (from a layman’s perspective) faced by victims of domestic violence and examines the associated factors (viz. structural, socio- economic factors and other risk factors) which perpetuate violence. Lastly, with the help of literature the paper has attempted to understand the extent of impact the Covid 19 pandemic may have had on the Indian women’s lived experiences of domestic violence and their mental health.
Methodology
This qualitative study was conducted in Munirka village. The topic being sensitive, it took time to build trust and rapport to conduct the interviews and only a small sample of thirty-eight women participants were part of the study. The participants were interviewed with the help of a self-designed in-depth interview (IDI) schedule and focused group discussions (FGD) were conducted for a more nuanced understanding of the topic. The IDIs and FGDs were conducted using IDIs and FGD guides that had been approved by the Ethics Committee (Anthropos India Foundation). The data was mainly collected offline, with help of community-based NGOs (CHERO India and Four B foundation) working with women between the age groups of 18-56 years in an urban village (Munirka) in south Delhi. Data were collected. The field investigators were trained about the sensitivity involved in the study and it was preferred that the investigators are either from the same locality if possible or otherwise have detailed knowledge about how to deal with such a sensitive topic. Considering gender sensitivity only women investigators conducted the IDIs and FGDs. In-depth interviews and FGDs were held at the convenience of the women in terms of time and location, and were audio recorded if permitted; otherwise, notes were taken.
As the data collection was conducted during the pandemic period all safety guidelines were followed with an emphasis on Covid appropriate behaviour. All the recorded interviews and focus group discussions were transcribed and translated. Qualitative [IDI (20) and FGD (08)] data were analyzed using coding and categorization, theme searching, validation of thematic analysis, and theme integration into the phenomenon under study.
Results and Findings
Research suggests that one out in three women across the globe experience domestic violence and almost 27% of women aged 15-49 having been in a relationship report being subjected to some form of physical and/or sexual violence by their intimate partner (WHO, 2024). 86.8% of our study sample also were between the ages of 18-45 years while 60.5% of the sample were between the ages of 18 to 35. Hence, this
Table 2: Socio-demographic and economic profile of the study area
|
Age in completed years of the respondent |
Delhi (%) |
|
18 to 25 years |
10.5 |
|
25 to 35 years |
50.0 |
|
35 to 45 years |
26.3 |
|
45 to 55 years |
13.2 |
|
Age in completed years study population |
|
|
0 |
2.6 |
|
>5 years |
5.3 |
|
5 to 10 years |
23.7 |
|
10 to 15 years |
28.9 |
|
15 to 20 years |
7.9 |
|
20 to 25 years |
15.8 |
|
<25 years |
15.8 |
|
Literacy rate |
|
|
Yes |
68.4 |
|
Completed education in years |
|
|
Not reported |
57.9 |
|
Primary |
2.6 |
|
Middle |
13.2 |
|
Secondary |
15.8 |
|
Senior secondary |
7.9 |
|
Graduation and above |
2.6 |
|
Occupation |
|
|
Not reported |
2.6 |
|
Business |
2.6 |
|
Domestic daily wage labour |
7.9 |
|
Regular wage salary earner |
2.6 |
|
Housemaid |
7.9 |
Source: Fieldwork data
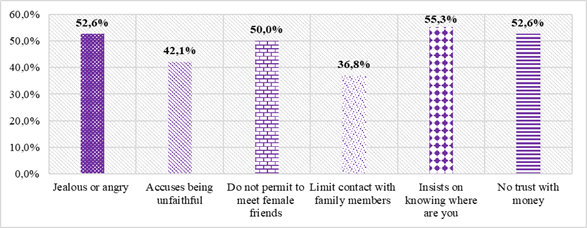
Relationship with Husband
Overall, (53%) of women said that their husband was jealous or angry when they talked with other men. About 42% said that their husband accused them of being unfaithful, almost 50 % of women reported restrictions faced in meeting female friends, 37% said that their husband did not allow them to meet family, 55% said that their husband insisted on knowing where they are at all times and 53% said that their husbands lacked trust (Figure 1). The women interviewed were primarily from the lowest economic strata, and as a result, they are less likely to resist violence. They understand that there is no other way to live their lives and internalise it. If they marry a man, it is entirely his decision what he does with her, and neither her parents nor anyone else can help her with this. Sonam (name Changed) is women of around 23-year-old and mother to three children living with her husband in a rent house in the Munirka urban village said that-
“Her husband is envious when she talks to other men, accuses her of infidelity, and refuses to let her see her friends. He frequently humiliates her in front of others, threatens to hurt and harm her, and occasionally insults and makes her feel bad about herself. She has been subjected to severe physical and psychological abuse. Sexual violence includes being pushed, shaken off, twisting her arm, and pulling her hair, being slapped, punched in the face, kicked, and dragged, and attempting to choke her throat and burn her. She has also been forced to perform unwanted sexual acts. As a result of domestic violence she has faced cuts, bruises, deep wounds and broke her bone”.
Another 32 years old respondent said that -
“My mother was beaten up by my father when I was a child, and we are three sisters. Our mother taught us that whatever your husband does is for your own good, and that he has the authority to beat you while taking care of your needs. We've always been told that no 42 person will ever help us and that anyone who does will pay a high price. Furthermore, women are there to serve their husbands, just as all the goddesses do for their god husbands”.
Figure 1: Relationship with husband
Source: Fieldwork data
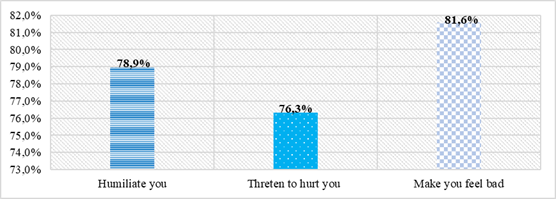
Incidents of humiliation and violence
Out of sampled (38) women, 82% of respondents reported that their husbands torture them mentally without any regrets. About 70% of women reported that they faced humiliation at the hands of their husband and 76% of respondents were threatened to get hurt by their husband (Figure 2). The FGD 2 reflected on this issue very clearly the following-
“While discussed with women’s in the group, it was found that many of them had attempted suicide. They were tired of their current situation. Domestic violence causes both physical and mental harm. They were suffering from both physical and mental illnesses. The women have been beaten to the point where they no longer believe they will live. Many of the interviews revealed that women are both mentally and physically oppressed, but their children are their only hope for a better life, and they will tolerate any type of oppression for the sake of their children…”.
Another 35 years old respondents reported that-
“According to the respondent, her relationship with another male friend was a mistake. She has repeatedly apologised to her husband for this, but he has lost faith in her. He forbids her from leaving the house without his permission and from meeting friends and family. She claims that her husband has never hit, slapped, or punched her, but he continues to verbally abuse and insult her about her extramarital affair”.
Figure 2: Incident of Humiliation and violence
Source: Fieldwork data
Incidents of physical and sexual violence
All the women reported experiencing violence at the hands of their husbands at some point in their life. 76% of women reported being slapped, 71% said that they were pushed, 58% reported that their husband twisted their arm, 58% were punched, 55% reported being kicked, 45% were choked and 40% of the sampled women said that they were threatened to be attacked by their husband (Table 3).
One of the respondents said that-
“My husband drink alcohol frequently but most of the time he is angry and if he demands anything and I could not fulfil because of any reason he starts beating me like animals. He beats me so much so that I am not able to get up, all my bangles broke. In covid he did not go for work, and he harassed me physically and mental on regular basis”.
The study also tried to capture the incidence of forced sexual intercourse faced by women. Only 21% of women said that they were physically forced to have sexual intercourse. State-wise average differences in the incidence of physical and sexual violence are below (Table 3).
Table 3: Incident of physical and sexual violence
|
Indicators |
Delhi (%) |
|
Push |
71.1 |
|
Twist Arm |
57.9 |
|
Slap |
76.3 |
|
Puch |
57.9 |
|
Kick |
55.3 |
|
Choke |
44.7 |
|
Threaten to attack |
39.5 |
|
Physical force to sexual intercourse |
21.1 |
|
Force to perform any other sexual act |
10.5 |
|
Force with threats to perform other way of sexual act |
7.9 |
Source: Fieldwork data
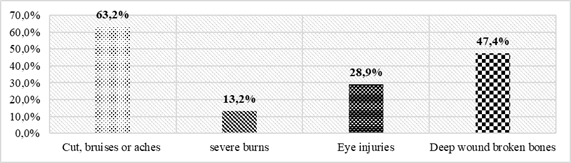
Physical injuries
As a result of physical and sexual violence, women's physical and mental health had been adversely affected. About 63% of women sustained cuts and bruises, 13% had severe burns, 29% had suffered eye injuries because of the violent acts of the husbands and 47.4% had deep wounds and broken bones. From among the sample only 4% of women reported having sometimes retaliated to their husbands’ acts of violence while no women reported initiating the physical or sexual assault (Figure 3).
Figure 3: Physical injuries
Source: Fieldwork data
Reasons for the domestic violence
The key reason for domestic violence was reported as drinking alcohol (40%) and lack of money (32%). Other less prevalent reasons include extramarital affairs (15%), bad habits (6%) and 7% of respondents had mentioned other issues. The fear profiles of victims of domestic violence are largely socially constructed and part of everyday life. Women are portrayed as being unable to make their own decisions and being forced to merely live up to others' expectations. One of the 33-year-old respondent reported that-
“He will beat me whenever he's drunk and feels like it; he doesn't need an excuse. It depends on his mood, and he keeps telling me that I don't understand his needs; he has beaten me if the curry was salty, he has beaten me when children cry, he has beaten me when the meal was late, and he has even beaten me if I woke up late in the morning. I don't say anything because if I do, the situation will deteriorate, and I will be beaten to death”.
In our patriarchal society girls have always been presented as a burden or a liability for the family and if anything goes wrong from the stereotype, a woman has to face the consequences. A man understands that the societal value of a woman is always less than a man. Taking the advantage of these facts, he shows his masculinity by physically harassing his wife.
In her own words a distressed woman upon asking that why she did not register police complaint against her husband narrated-
“If I lodge complaint in police or dare to resist his beating, where would I go? He is the sole breadwinner of the family. Who doesn't get beaten up by husband? He is the one who is feeding us, he can beat us too. Moreover, if police take him to jail he will lose his one day wage and that will cost on the whole family”
Another respondent said that-
“My husband do not drink alcohol frequently but most of the time he is angry and if he demands anything and I could not fulfil because of any reason he start beating me like animals.He beat me so much so that I am not able to get up, all my bangles broke”.
Upon asking that why she does not take any help from anyone in such case her reply was-
“Who should I complaint if my husband whom I am married is culprit who will listen to me. He is the one who takes care of everything, who earns and feed us. Sometimes I feel like running away from this house then thought of my kids don’t let me do so. I cannot go to my parents’ house as I have three more sisters who are yet to be married and my father is a daily wage laborer”.
Financial deprivation was a common practice used by men to gain control of women. Women complained that their husbands spent whatever money they earned on alcohol and left little or no money for household expenses. One of the main reasons why most of the women were stressed and malnourished was because of this. According to the data, men spend approximately 70 to 80 percent of their earnings on alcohol, while only 20 to 30 percent is used for household expenses. Women were afraid of being excluded if they did not follow the rules of the community/society, i.e. in a society, a woman is believed to be a servant of her husband and to seal her lips against whatever happens to her. FGD two discussion, where most of women concern that-
“We're being beaten up, but no one stands with us; instead, they point their finger at us, as if we've done something wrong. Others argue that whatever happens, he is your husband, and you and your children rely solely on his earnings”.
Character assassination fear was another type of fear that nearly all the women mentioned. Women reported that they are frequently physically and verbally abused by their husbands under the pretext that they are having an extramarital affair. When asked, "Why do they do that?" They responded that their husbands don't trust them and believe that we get to indulge in all of these activities once they leave for work. In essence, it is a psychological phenomenon that men experience; after drinking, all of their senses become weekend, and they fall asleep because they are at ease. Thus, a person who sleeps almost 12 hours per day spends the other 12 hours working or engaging in other activities. Due to their inability to spend time with the family, mistrust develops.
One of the respondents in her own words-
“I have grown up seeing my mother being beaten up by my father and we are three sisters. Our mother has taught us that whatever your husband does it is for your own good and after all he has the authority to beat you as he takes care of your need. We have always been told that no one will help forever and anyone else help us they will take a heavy price. Moreover, women are there to serve their husband; even all the goddess does the same to their god husbands”.
Women’s views on alcoholism
The study also captured women's views on alcoholism and how it affects their family life. Every 7 out of 10 of the sampled women knew about the health hazards of alcohol consumption. More than half of them (61%) reported an incidence of death in the community due to alcohol consumption (Table 4). Majority of the respondents mentioned that “Alcohol consumption is not good for health” and “Alcohol leads to domestic violence” (Table 4). This was further strengthened in the FGD-3 as follows:
“One of the major perpetrators of this crime triad is the unregulated sale of alcohol in the community. Many of the women have stated that if there had been no alcohol, they would not have been subjected to as much violence. Some believe that men are more violent by nature than women. Many of the women pointed to their husbands' bad behaviour”.
Table 4: Women views on alcoholism and its impact on family life
|
Indicators |
Delhi (%) |
|
Do you know alcohol case |
71.1 |
|
Is there any death |
60.5 |
|
Husband drink alcohol |
89.5 |
|
Often husband drink alcohol |
|
|
Often |
55.3 |
|
Sometime |
36.8 |
|
Not at all |
7.9 |
|
Things that husband does after drinking alcohol |
|
|
Not answered by the respondent |
28.9 |
|
Fight/shout |
36.8 |
|
Physical abuse |
28.9 |
|
Physical hit |
5.3 |
Source: Fieldwork data
Regarding alcohol consumption, the data shows 55% respondents reported their husband consumed alcohol very often, 37% consumed alcohol sometime while only 8% reported no consumption. Data shows 37% respondents reported their husband fought/shouted and 29% were abused by them after consuming alcohol. Men were reported as having spent money on alcohol despite tough times such as COVID 19 and unemployment by taking loans or spending family savings. Data suggests 63.2% men often spent on alcohol consumption while 30.9% men spent sometimes on purchase of alcohol. (Table 4). About 29.4% of men would take money from their wives or family savings. This led to fights within the family leading to domestic violence. The FGD-3 also gave similar indications-
“Primary reason for domestic violence is alcohol consumption by husband who gets angry over small things leading to extreme violence. Husbands drink alcohol regularly and spend more than his monthly earnings on purchase of alcohol. They think that selling alcohol should be banned as it leads to violence and creates money related problems”.
The mental health status of Women
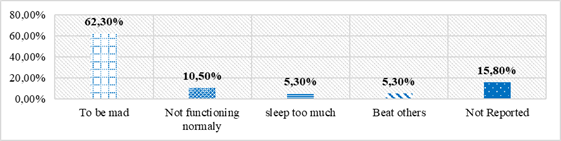
Mental health
Aside from alcoholism and domestic violence, respondents were asked about their mental health knowledge, mental disorders, treatment location, and if they had ever suffered from any mental health problem. In total, 74% of respondents reported being aware about mental health, while the rest had no knowledge. Then the question was asked about the meaning of mental health. In response to questions on the meaning of mental health a higher percentage (63%) of respondents reported mental health to them meant to be mad, followed by not being able to function normally (10%), to sleep too much (5%), while 5% indicated beating others means having mental health problems. Data revealed that misconceptions are still prevailing among the respondents about issues of mental health and wellbeing while there was familiarity with terms such as depression and dementia. However, there was a lack of clear understanding of the differentiation between mental health and mental disorder and they were tended to be equated. Most respondents also understood mental health as being mad/madness (Figure 4).
Figure 4: Knowledge on meaning of mental health and mental disorder
Source: Fieldwork data
Information on mental disorder and source of knowledge
Those with some awareness about mental health problems/disorders were asked if they had received information about mental health problems. In response, 76% of respondents said they had received information about depression, 11% received information about dementia, and 8% had received information on bipolar affective disorder. The survey found that respondents received information about mental health problems from friends 23%, 21% from family, 10% from local doctors at CHC and PHC level, 10% obtained from television, and 10% received information from other sources such as (Table 5).
Table 5: Received information on mental disorder and source of knowledge about mental health
|
Received information on mental disorder |
Delhi (%) |
|
Depression |
76.3 |
|
Dementia |
10.5 |
|
Bipolar affective disorder |
7.9 |
Source: Fieldwork data
Feeling of restlessness and its reasons
Data presented in Table 6 showed that 60% respondents reported they feel restless and are unable to work sometime while around 40% respondents reported feeling restless and always unable to work (Table 6). One of the 27 years old respondents reported that-
“I feel very restless...I feel tired and sleepy… have little money to buy anything for home or myself... and he (husband) beats up whenever he feels like it... 'Drinking is frequently used as an excuse…”
Similarly other respondents reported mental health as difficulty functioning normally and reported feeling restless almost always mostly due to personal health (Radhika); spousal violence (Sahzia); and economic hardship (Salima). A variety of reasons were given by the respondents for feeling restless, 58% said that it is because of physical health, 32% reported it is related to household’s poor economic condition. 7% reported that it is because of social reasons and 4% reported that is related to non-availability of support system. Among those who felt restless, only 58% reported having consulted with anyone for support. All the respondents consulted with friends, family members, local doctors, whereas 32% of women consulted with family, 26% consulted with local doctors and 5% consulted with friends to cope with mental health problems. One of the respondents said that-
“She has not received any information about mental health disorders. She occasionally feels restless, but she has not consulted a doctor because she believes her restlessness is caused by weakness. She does not practice any recreational activity other than worshipping god and cooking.”.
Table 6: Mental health and restlessness
|
Feel restless and are unable to work sometimes |
Delhi (%) |
|
Always |
39.5 |
|
Sometimes |
60.5 |
|
Reasons for feeling restless |
|
|
Physical health |
58.4 |
|
Social reasons or events |
6.6 |
|
Reasons related economy |
31.7 |
|
Non-availability of support system |
4.3 |
|
Consult with anyone for support to cope with the situation |
|
|
Yes |
57.9 |
|
Discussed with whom about the situation |
|
|
Not reported |
31.6 |
|
Family members |
31.6 |
|
Friends |
5.3 |
|
Local doctor at CHC/PHC |
26.3 |
|
Any others |
5.3 |
Source: Fieldwork data
The data analysis is indicative of the following type of behavioral/ psychological change that women adopt after being beaten or threatened by their partners.
Low self esteem
All the women involved in the study showed low self-esteem. They shared their life stories of being beaten and harassed by the partner and at the same time they accepted it as their destiny. The study registers that domestic violence is very much socially structured and is part of the patriarchy mindset. A subtle understanding was prevalent among all the respondents that a woman needs a man for survival. This perception was so strong among the women that while interviewing them they mentioned it several time -
I am married to him and now he is everything to me.
Women lacked self-esteem to the extent that they could not imagine their life without their husband. They have internalized the fact that it is a curse to be born as a girl as you don’t have anything of yours. This internalization comes through the social process that an individual goes through her life.
Suicidal ideation
This means that when someone is preoccupied with the idea of suicide. One may regularly think about the way he/she would commit suicide or think about what life would be like if he/she wasn’t around. One may also replay the suicidal act out in his/her mind. Around 70 percent of the women showed suicidal ideation and many of them have even attempted suicide for more than one time. While talking to the women it was noted that many of the women have tried to kill themselves. They were frustrated and tired of the life they were living. These women, as victims of domestic violence, suffered not only physical discomfort but their mental health suffered as well. The women are beaten up to an extent that they lose all hope of living. In many of the interviews it was found women are severely oppressed, harassed both mentally and physically but their children are their hope of life, and they tolerate all types of oppression for the sake of children. It was also noted that many of the women were continuing with their marriage due to their children as they could not think of alternate avenues for housing or financial security.
Constant fear
The women as victims of domestic violence are under constant fear, fear of being beaten. Fear of being abandoned, fear of being economically deprived, fear of being excluded, fear of being sexually assaulted, fear of character assassination, fear of shame and list goes on. It is a general mindset and in fact a psychological practice that if one wants his subordinate to always be subordinate, he/ she will never make him comfortable and will always keep him under constant fear. The fear lists of victims of domestic violence are very much socially constructed and are part of daily life. The situation of women is reduced to being merely a person who is just working for others' expectations and has no option to make choices. The constant fear of being beaten up was the most common fear that almost all the women respondents reported. The women were not sure that why they are being beaten up and it was very surprising that they said-
“Whenever he is drunk and feels like beating, he will beat me, he doesn’t need any excuse.
And sometime even if he is not drunk, he will beat. It depends on his mood, and he keep telling me that I don’t understand his needs, he has beaten me if the curry was salty, he has beaten me children are crying, he has beaten me if there was delay in serving meal, he has even beaten me if I woke up late in the morning. I don’t say anything because if I say it then it will become worse, and I will be beaten till death”.
Financial deprivation was one of the common practices practiced by men in order to have control over the woman. Women complained that whatever their husbands earned, they buy alcohol out of it and give very little or no money for the household expenses. This was one of the major reasons that most of the women were stressed and malnourished. It was evident from the data that men spend around 70 to 80 percent of their earnings on alcohol and only 20 to 30 percent is for household use. The women feared of being excluded if they did not obey the community/societal rules. Most of the women showed this worry that –
“We are being beaten up still people doesn’t stand with us instead they point their figure towards us only, that we have only done something wrong. Other people say that whatever happens, but he is your husband and you and your children survive on his earning only.”
Women throughout the study have shown that they were sexually abused by their partners and in many cases, they were assaulted by other family members. The frequency of being sexually assaulted was higher among those with alcoholic husbands than the non-alcoholic ones. Although it was difficult for the women to call it assault as they assume that the husband has full right on their body, and it is their wish how they want to behave with it. In their words-
“Marriage legitimizes all kind of bodily involvement with each other, even if they don’t.
wish to be involved”.
According to some participants, there was no resistance to their husband’s demand as it could result in grave injuries or violent consequences. Another kind of fear that most talked about was the fear of character assassination. Women revealed that most of the time they are beaten by their husbands on the pretext of suspicion of an extramarital affair. On further probing, they said that their husbands don’t trust them and think that after they leave for work the women indulge in such activities.
A participant explained this aptly –
“basically, it is a psychological phenomenon that the men exhibit, after consuming alcohol all their senses are weakened and they sleep as they feel relaxed. So a person who is sleeping almost 12 hours a day and remaining 12 hours is spent either in working or in doing something else. So, they are not able to spend time with the family and therefore the distrust arises.”
Discussion and conclusion
Some specific findings of the study indicate that in Delhi there were rising cases of broken marriages as a result of domestic violence and alcoholism. There was no support available, or the victims had no access to information about the support available. Furthermore, the police were also found to be ineffective. The women appeared to be trapped in a stereotypical and vicious cycle of poverty, financial insecurity, strict patriarchal norms, weakened mental state, fear associated with display of any resistance, etc. Findings also highlighted the suspicions and character assassination carried out by the husbands. While character assassination is the simplest form of abuse a perpetrator can do in order to prove himself right, it takes everything for a woman to prove herself innocent. Even if a woman smiles while talking to anyone she was tagged as a woman of bad character. The women were often accused of betraying their husband, even by the men in the community. Such allegations were made on the basis of assumptions and suspicions. Similarly, Bhandari & Hughes (2017) also state that women experience prolonged periods of violence due to shame on their families or themselves and/or because of little to no social and financial support.
Most of the women during FGD reported that reasons for violence were alcoholism among men which leads to beating, money related issues, small fights that trigger violence, men doubting women unfaithful, and violence caused due to unemployment. Among all reasons alcohol consumption was reported as the main reason for domestic violence. Especially in the face of COVID-19 it may be noted that due to extended lockdowns and confined living conditions domestic violence, especially IPV, cases were on the rise and this was reported from across the globe (Kumar, 2020) being perpetuated by money, health and security concerns. Sardinha et al., (2022) noted that violence against women by male intimate partners is a global public health concern with long and short term, physical and mental health impact on women and children.
Women said that domestic violence can occur with any woman irrespective of caste or socioeconomic status. However, among women of low socioeconomic status domestic violence is very common and there are more reported cases. Ramasubramani et al. (2024) also found that women with low education, being employed, husband being uneducated or with coercive behavior had significantly higher prevalence of domestic violence.
There are serious mental health issues among victim women that go unnoticed, creating a vicious cycle. A study on Indian women is indicative of significant positive correlation between domestic violence, depressive and anxiety symptoms and domestic violence was a significant predictor of depressive and anxiety symptoms in this population, after adjusting for other variables (Indu et al., 2021).
The study has a limitation wherein the fieldwork was conducted during Covid 19 and although the data may not be equipped to corroborate the impact of Covid 19 on the instances of domestic violence against women and their mental health, subsequent literature has established the relationship between domestic violence, mental health and Covid 19. Hence, the violence realm can be drawn from subsequent literature that establishes the relationship with Covid 19. Hence, the study provides baseline information on how Covid 19 may have impacted women’s health by aggravating their lived experiences. While violence and mental health concerns already existed in the lives of these women the study highlights how Covid could have behaved and resulted in aggravating the lived experiences of women. Future research may also examine long-term trends of alcohol-use, domestic violence, and mental health. While this paper has focused on the women victims’ it may also be prudent to have a more balanced understanding of both men and women as victims of domestic violence.
In conclusion, our study indicates that there is a need for amplification of women’s voices, choices, and agency to fight against a social ill like domestic violence. In line with existing literature, our study observed that domestic violence not only impacts physical health but also has bearings on one's mental health. Domestic violence is also said to cause women to be isolated, unable to work, loss of wages, lack of participation in regular activities and limited ability to care for themselves and their children (WHO, 2024). Hence, the issue of domestic violence is not purely medical and nor can it be treated as just a legal issue. Multiple agency engagement with a multi-disciplinary approach is crucial. Therefore, state, and non-state agencies, academicians and institutions will be required to be involved in empowering women economically for their financial sustenance and coping skills to deal with domestic violence. All health practitioners should be trained on aspects related to domestic violence, its physical and mental health impact. ANMs, community health workers should be trained on basic counselling skills as they visit women to give maternal health and immunisation care for children. The earlier the risks are identified the sooner the problems can be tackled.
Acknowledgement: The paper has been drawn out of a larger study on ”Alcoholism, mental health, domestic violence and coping strategies of women in Delhi slums, Rural UP, Rajasthan and Telangana: Finding tangible solutions for actions” sponsored by the National Commission for Women.
References:
Ali, P., Rogers, M., & Heward-Belle, S. (2021). COVID-19 and domestic violence: impact on mental health. Journal of criminal psychology , 11(3), 188-202.
Bhandari, S., & Hughes, J. C. (2017). Lived Experiences of Women Facing Domestic Violence in India. Journal of Social Work in the Global Community , 2(1). https://doi.org/10.5590/JSWGC.2017.02.1.02
Dawson, D. A., Grant, B. F., Chou, S. P., & Stinson, F. S. (2007). The Impact of Partner Alcohol Problems on Women’s Physical and Mental Health. Journal of Studies on Alcohol and Drugs , 68(1), 66–75. https://doi.org/10.15288/jsad.2007.68.66
Gadd, D., Henderson, J., Radcliffe, P., Stephens-Lewis, D., Johnson, A., & Gilchrist, G. (2019). The Dynamics of Domestic Abuse and Drug and Alcohol Dependency. The British Journal of Criminology , 59(5), 1035–1053. https://doi.org/10.1093/bjc/azz011
Ghosh, S. (2015). The Political Economy of Domestic Violence in a Mumbai Slum: An Ethnographic Analysis. Journal of Interdisciplinary Economics , 27(2), 175-198.
Golder, S. (2016). Measurement of Domestic Violence in NFHS Surveys and Some Evidence . Retrieved from https://oxfamilibrary.openrepository.com/bitstream/handle/10546/620102/wp-measurement-of-domestic-violence-in-nfhs-and-some-evidence-230816-en.pdf?sequence=1
Indu, P. V., Vijayan, B., Tharayil, H. M., Ayirolimeethal, A., & Vidyadharan, V. (2021). Domestic violence and psychological problems in married women during COVID-19 pandemic and lockdown: a community-based survey. Asian journal of psychiatry , 64, 102812.
Kalokhe, A., del Rio, C., Dunkle, K., Stephenson, R., Metheny, N., Paranjape, A., & Sahay, S. (2017). Domestic violence against women in India: A systematic review of a decade of quantitative studies. Global Public Health , 12(4), 498–513. https://doi.org/10.1080/17441692.2015.1119293
Kourti, A., Stavridou, A., Panagouli, E., Psaltopoulou, T., Spiliopoulou, C., Tsolia, M., Sergentanis, T. N., & Tsitsika, A. (2023). Domestic Violence During the COVID-19 Pandemic: A Systematic Review. Trauma, Violence, & Abuse , 24(2), 719-745. https://doi.org/10.1177/15248380211038690
Kumar, A. (2020). COVID-19 and domestic violence: a possible public health crisis. Journal of Health Management , 22(2), 192-196.
National Family Health Survey-3 (2006). Domestic Violence . Retrieved from http://hetv.org/india/nfhs/nfhs3/NFHS-3-Chapter-15-Domestic-Violence.pdf
National Family and Health Survey. (2019–2021). India fact sheet. National Family and Health, Survey (NFHS-5) . International Institute of Population Sciences. Retrieved from http://rchiips.org/nfhs/factsheet_NFHS-5.shtml
National Crime Records Bureau. (2021). Crime in India . Retrieved from https://data.gov.in/ministrydepartment/National%20Crime%20Records%20Bureau%20(NCRB)
National Commission for Women. (2023). Retrieved from https://ncwapps.nic.in/pdfReports/AnnualReport2022_2023_Eng.pdf
Pandey, A., & Nath, D. C. (2014). Correlates of Domestic Violence in India. GSTF Journal of Law and Social Sciences (JLSS), 4(1), 1.
Ramasubramani, P., Krishnamoorthy, Y., Vijayakumar, K., & Rushender, R. (2024). Burden, trend and determinants of various forms of domestic violence among reproductive age-group women in India: findings from nationally representative surveys. Journal of Public Health , 46(1), e1-e14.
Raj, A., Saggurti, N., Lawrence, D., Balaiah, D., & Silverman, J. G. (2010). Association between adolescent marriage and marital violence among young adult women in India. International Journal of Gynecology & Obstetrics , 110(1), 35-39.
Sardinha, L., Maheu-Giroux, M., Stöckl, H., Meyer, S. R., & García-Moreno, C. (2022). Global, regional, and national prevalence estimates of physical or sexual, or both, intimate partner violence against women in 2018. The Lancet , 399(10327), 803-813.
Scheper-Hughes, N., & Bourgois, P. I. (Eds.). (2004). Violence in war and peace: An anthology (Vol. 5). Blackwell Pub.
Sinha, A., Mallik, S., Sanyal, D., Dasgupta, S., Pal, D., & Mukherjee, A. (2012). Domestic violence among ever married women of reproductive age group in a slum area of Kolkata. Indian journal of public health , 56(1), 31.
Srivastava, D. K., Mishra, A., Patne, S. K., Tiwari, R., Gour, N., & Bansal, M. (2014). A cross-sectional study to find out the prevalence of different types of domestic violence in Gwalior city and to identify the various risk and protective factors for domestic violence. Indian journal of community medicine, 39(1), 21.
Su, Z., McDonnell, D., Roth, S. et al. Mental health solutions for domestic violence victims amid COVID-19 (2021): a review of the literature. Global Health 17, 67, https://doi.org/10.1186/s12992-021-00710-7
Visaria, L. (1999). Violence against women in India: Evidence from rural Gujarat. Domestic violence in India. Washington: International Center for Research on Women , 999, 9-7.
Vora M, Malathesh BC, Das S, Chatterjee SS. COVID-19 and domestic violence against women. Asian J Psychiatr. 2020 Oct; 53:102227. doi: 10.1016/j.ajp.2020.102227.
Wilson, B., & Butler, L. D. (2014). Running a gauntlet: A review of victimization and violence in the pre-entry, post-entry, and peri-/post-exit periods of commercial sexual exploitation. Psychological trauma: theory, research, practice, and policy, 6 (5), 494.
World Health Organization. (2022). Alcohol . Retrieved on 10-07-2022 https://www.who.int/news-room/fact-sheets/detail/alcohol
World Health Organization. (2024). Violence against Women . Retrieved on 04-05-2024. https://www.who.int/news-room/fact-sheets/detail/violence-against-women
Yasmin, M., Gådin, K. G., Viitasara, E., & Dalal, K. (2022). Prevalence and correlates of domestic violence against ever married women of reproductive age in India: changes during 2005-2015. Journal of Injury and Violence Research, 14(3), 153.
Author´s
Address:
Ajit Kumar Lenka
Assistant Professor at the Department of Public Health, Noida International
University, Uttar Pradesh, India
ajitlenka.lenka@gmail.com
Author´s
Address:
Neha Sharawat
Research scholar at the Department of Food Science and Nutrition, Banasthali Vidyapith, Rajasthan, India
nehaasahrawat@gmail.com
Author´s
Address:
Smritima Diksha Lama
Japan Foundation
Indo-Pacific Partnership Research Fellow, Graduate School of Social
Sciences, Hitotsubashi University, Tokyo (Japan)
smritima@gmail.com
Author´s
Address:
Sanghmitra S Acharya
Professor and Head at the Centre of Social Medicine and Community Health, Jawaharlal Nehru
University, New Delhi
sanghmitra.acharya@gmail.com