Health Financing and Equity in Healthcare for Disadvantaged Groups in Vietnam
Thi Xuan Huong Le, University of Labour and Social Affairs
Thi Hai Duong Nguyen, National Economics University
Thi Thuy Dung Nguyen, Military Hospital 103
Thi Huu Ai Nguyen, University of Labour and Social Affairs
Thi Huong Tram Le, University of Labour and Social Affairs
Nguyen Zen Nguyen, University of Labour and Social Affairs
Abstract: Equity in health means that all people in general and disadvantaged groups in particular receive the same healthcare services, according to their needs, regardless of each person's financial ability and social status. In Vietnam, equity in healthcare for the disadvantaged is expressed in the Party's guiding viewpoints, guidelines, and legal policies. This study has employed a combination of quantitative and qualitative research methods to understand the impact of health financing in advancing health equity for disadvantaged people. Quantitative and qualitative research methods have helped us evaluate the current health financing and equity in healthcare for disadvantaged people in Vietnam. The study assessed the health financing activities, including the distribution of free health insurance cards to disadvantaged groups, medical examination and treatment available, and the services of social workers at hospitals and localities. Based on the results of this analysis, we identify existing gaps and their causes. Based on the findings we build and propose solutions for government agencies, training activities, medical facilities, and social work organizations. The significance of the proposed solutions is to improve fairness and efficiency in financial use and healthcare for disadvantaged groups in Vietnam.
Keywords: Disadvantaged groups; Fair; Healthcare; Health finance; Vietnam
1 Introduction
Health finance has the role of allocating financial resources to pay for health services, meeting the healthcare needs of people and society. In Vietnam, fairness in the distribution of medical services is the operating goal of the health financing system. To improve fairness in people's healthcare, the Vietnamese government and social work organizations have many policies to support people, especially disadvantaged groups. This group includes older adults, the poor, people with disabilities, ethnic minorities, people infected with HIV/AIDS, and gay, bisexual, and transgender groups (Vietnam Social Security [VSS], 2017, para.1). Because disadvantaged groups have many difficulties in accessing basic needs, they need psychological and financial support from the government and social work organizations. Vietnam has used tax resources to provide free health insurance cards to disadvantaged groups. In addition to the policy of eliminating diseases, building facilities, and consolidating and perfecting the grassroots medical network, Vietnam also has many policies to financially support medical examination and treatment for the poor, ethnic minorities, and other disadvantaged groups, ensuring equity in healthcare. Social work activities at medical facilities have been promoted, and many patients in disadvantaged groups have received psychological support and financial support when they suffer from critical illnesses. Social workers have encouraged people infected with HIV, gay people, and transgender people to overcome psychological obstacles and receive treatment at medical facilities. Combining financial support measures, favorable legal corridors and effective social work activities, Health Insurance in Vietnam has covered 92.04% of the population (Ministry of Health [MOH], 2023, para1). Although some positive results have been achieved, equity in healthcare for disadvantaged groups in Vietnam is still not guaranteed. The reason is that disadvantaged groups mainly live in rural and mountainous areas and do not have the conditions to take advantage of benefits from health insurance (Quyen, 2019, p.2). There is a shortage of social workers in Vietnam, so they can only support a few disadvantaged people when they are discovered coming for medical examination and treatment at medical facilities. Meanwhile, in rural and mountainous areas, many disadvantaged people have never gone to a medical facility because of guilt, and they have not received the necessary medical care. Although efforts to extend medical facilities in rural and mountainous areas are in progress, operating conditions are difficult, and equipment is lacking synchrony. Doctors with high professional qualifications do not want to work in underdeveloped areas, so disadvantaged groups have difficulty accessing quality medical examination and treatment services. Although disadvantaged groups have been supported with inpatient examination and treatment costs, Vietnam's medical financial resources are not enough to fully support all costs, especially for groups with critical illnesses. Although social work activities at the hospital have called for support for some patients, this funding is still limited. At this time, to treat the disease, disadvantaged groups still need to pay from their own pockets or give up treatment when they cannot afford to pay. The above causes have indirectly caused inequality in the distribution of healthcare services among people. In addition, there is a large proportion of older adults in disadvantaged groups who are not eligible for free health insurance cards and are living in rural, and remote areas. They have difficulty buying voluntary health insurance cards because the cost is highly unaffordable, as their income is often meager. This means that low-income older adults have to spend a significantly higher proportion of their income to obtain health insurance cards than their affluent counterparts, leading to inequity in health financing. The goal of this study is to understand the theoretical basis of health financing and equity in healthcare for disadvantaged groups. By evaluating the effectiveness of health financing and equity in healthcare for disadvantaged groups in Vietnam, the study seeks to identify solutions and propose recommendations to the government, medical facilities, and social work organizations to improve equity in healthcare for disadvantaged groups in Vietnam.
2 Theoretical basis
2.1 Health finance
Vietnam does not have a unified definition of health financing. When we talk about health financing, we are talking about the allocation of funding sources to medical facilities, payment of medical service costs, and labor costs for individuals participating in the delivery system of social healthcare services (Chuc, 2007, p.74). Gapenski & Reiter (2012) also states that "Health finance does not have a single answer, the definition of health finance depends on the context in which it is used" (p.4). Health finance is an important part of the health system. This system has three main goals: Mobilize enough financial resources for the development of the health sector and people's healthcare; Manage and allocate resources towards fairness, efficiency, and development; Improve professional quality and technical development in providing medical services (Hai, 2016; p.7). According to the World Health Organization [WHO], health financing is a basic and important function of the health system. Health finance performs the function of gathering and prudently disbursing financial resources to pay for health services and meet the healthcare needs of people and society. WHO also emphasizes the need for providing access to healthcare services and the importance of allocating necessary financial resources to provide this healthcare access to people, thereby promoting universal health coverage (WHO, n.d.).
The health financing system in many countries around the world has different methods of raising financial resources for healthcare services, mostly through public and private financial sources. Public financial resources are raised from the Government or from the state-run Social Health Insurance to pay for medical costs. Private financial sources involve paying medical expenses from the patient's pocket or through private health insurance. The disadvantage of private finance is that it can hinder and limit patients from disadvantaged groups and low-income groups from accessing medical services when they do not have enough financial resources and are at risk of poverty. Public finance, funded by the state, pays for health services based on medical examination and treatment needs, enabling easier access to health services for weaker sections of society. In Vietnam, Social Health Insurance has been implemented since 1992 and is considered the main method of public financing for healthcare. Vietnam's health finance is formed based on health financial resources from the State Budget, aid sources, health financial resources from Social Insurance and health financial resources from outside the State Budget (MOH, 2008, p.20).
Thus, although health finance does not have a specific definition, it involves raising financial resources for healthcare needs and distributing them appropriately to serve the community's healthcare goals.
2.2 Disadvantaged group
The term “disadvantaged person” is considered a legal term. Quyet & Tuan (n.d, p.1) state that “The term disadvantaged has been traditionally used as an adjective as if to describe an inherent quality of the group as weak and disadvantaged”. In addition, these authors also identify that the term as a verb, to refer to a process in which the social behaviors of a particular group are carried out in a certain way, completely "unfavorable" for them (para.2). In his research on the social adaptation of disadvantaged social groups in Vietnam, Dung (2012) assessed that disadvantaged social groups are special social groups. They are often people who face many difficulties in daily life, and social activities. The author makes specific comments regarding the group of children, who do not have enough life experience and do not meet physical requirements. For the elderly and sick people, they face difficulties in health and illness. For the group of people with disabilities, it is a physical deficiency or defect (p.2). Bac (2023) believed that "disadvantaged people are people whose natural abilities are partly limited or due to social factors that cause them to be underestimated in terms of status in economic and political fields" political and social in the same circumstances, conditions, and available capabilities” (p.1). He also states that Vietnamese law recognizes people belonging to disadvantaged groups similar to international law. However, due to specific socio-economic factors, Vietnamese law also regulates several other subjects such as people living in particularly difficult circumstances due to poverty, disease and environmental impacts as well as belonging to disadvantaged groups (Bac, 2023,).
Thus, disadvantaged people are a legal category, but determining who belongs to this group depends on the perspective of each country, region, political environment and living environment. However, disadvantaged groups all have the common characteristic that they have difficult living conditions than the rest of the community. They have low social status and face many challenges in accessing healthcare, education, and employment. In addition, disadvantaged groups also encounter social discrimination and alienation, leading to psychological problems.
2.3 Equity in Healthcare
Document of the 11th National Congress of the Communist Party of Vietnam (2011) clearly stated that "The State must have political responsibility for healthcare for all its citizens, regardless of their health status." men, women, rich and poor, ethnicities, ages, and regions of the country. The foundation of that responsibility is humanitarianism, the philosophy of social justice" (pp.128-129). Evin (2003) believed that people are not equal before illness but can receive equality in accessing necessary medical care for themselves, even if their income level is not high. In research on solutions to implement equity in healthcare for Vietnamese people, Cuong (2005) stated how, "Equality in healthcare in Vietnam means that those with the most needs will be cared for … those who are disadvantaged (economically and socially) must receive more attention” (p.32). Therefore, Cuong (2005) concluded that health resources must be allocated based on healthcare needs, not on the ability to provide health services, and emphasized public health. Health equity is like welfare equity. The State must use equity in Welfare as a criterion to evaluate the results of health financial distribution activities. Quy (2015) believed that health equity is expressed through the perspective of equity in healthcare. It includes horizontal equity and vertical equity. Horizontal health equity is where people have different health needs but receive equivalent healthcare. Vertical health equity means that people with higher healthcare needs will receive more medical support. The document "Indicators for Monitoring and Evaluating Equity and Effectiveness in Healthcare" gives the opinion that equity in health is that all people receive the same healthcare services, not considering their financial capabilities and status in society. Poorer groups of people living in economically difficult areas will receive more support from the State (MOH, n.d., pp.6-9). “The concept of equity in healthcare does not mean equality. Talking about equity means giving priority to the poor, the meritorious, and the disadvantaged" (cited in Quy, 2015, para.3).
Thus, the studies we mentioned all give quite consistent conclusions about fairness in people's healthcare. Accordingly, fairness is the way people receive medical care according to their needs and health situation. The medical services that they are provided do not depend on their financial ability or social class.
2.4 Health financial allocation and equity in healthcare for disadvantaged people in Vietnam
The Vietnamese Government has used the state budget to provide free health insurance cards for disadvantaged groups of people as prescribed in Clause 3, Article 12 including children under 6 years old, older adults (80 years and above), people with disabilities, poor people according to the poverty line in the period 2022-2025 and ethnic minorities living in areas with difficult socio-economic conditions (Law on Health Insurance, 2014, p.3). Free issuance of health insurance cards also contributes to building a fair, effective, and sustainable health system. When disadvantaged people have health insurance cards, they will have the opportunity to access quality and safe medical services. This not only helps improve people's quality of life and health but also contributes to socio-economic development and social security. In addition to the use of finance, Vietnamese law also promulgates regulations on the tasks and forms of organizing the implementation of social work tasks in hospitals. The main tasks are to support and advise on solving social work problems for patients and their families during the medical examination and treatment process. The roles, hence, include communicating about policies and rights of patients in medical examination and treatment, enabling the community to support patients with special difficulties, psychological consultation, approaching, talking, and listening to patients with psychological problems such as stress, anxiety, and depression to help them relieve negative emotions and have confidence in the treatment process, carrying out charity activities and mobilizing and receiving financial and material donations to support patients in difficult circumstances. Social workers are also expected to guide social work students at social work training establishments; fostering and training knowledge about social work for medical and hospital staff.
3 Methods
3.1 Systematic review
We use the systematic review to build an overview of the theoretical basis of health finance, equity in healthcare, health finance allocation policies, and social work tasks at the hospital. Document research is a method of searching and synthesizing information and theoretical knowledge from available sources such as legal regulations, documents of health, labor and social management agencies, articles in magazines, and published research results of scientists related to the research problem. Specifically, we rely on WHO Vietnam's documents on health financing, the Health Sector Overview Report, and comments from authors with related research to draw a theoretical basis for health financing in Vietnam. For the theoretical basis of equity in healthcare for disadvantaged groups, we rely on the Ministry of Health's documents on the Index for monitoring and evaluating equity and efficiency in healthcare, and regulations in Laws, Circulars, and Decrees related to equity in healthcare such as the Health Insurance Law; Resolution No. 20-NQ/TW on ensuring equity in people's healthcare; The Circular regulates the tasks and forms of organizing social work tasks of hospitals or the Project for developing the social work profession in Vietnam.
3.2 Qualitative research
The qualitative data in the article is drawn from two sources: secondary sources and primary sources. We collected secondary data from the Ministry of Health, the Vietnam Social Insurance Agency, and the General Statistics Office. Specifically: Preliminary report on 5 years of implementing Resolution No. 96/NQ-BCS on innovating and improving the quality and effectiveness of social insurance and health insurance communication work; Report on health insurance coverage rates in provinces across the country; Socio-economic development report in 2022 according to Resolution No. 32/2021/QH15 on the target number of doctors/1,000 people and number of hospital beds; Report on the results of implementing the social work profession development project; Statistical indicators on labor and medical payments in the Vietnam Statistical Yearbook. In addition, some data were collected from studies published in Social Insurance magazine and Dan Dan magazine. Based on secondary data, we evaluate the allocation of medical finance, the issuance of free health insurance cards to disadvantaged people and the effectiveness of the policy of exemption and reduction of medical and treatment costs for diseases for disadvantaged people in Vietnam. These are activities aimed at equity in people's healthcare, especially disadvantaged people.
Primary data for the qualitative phase was collected through interviews. The content thus generated was used to evaluate the results of implementing the national set of criteria on commune health. The interviews covered 32 officials from 32 communes in 8 regions (Northwest, Northeast, Red River Delta, North Central, South Central, Central Highlands, Southeast and Mekong River Delta). The interview participants were managers in the commune-level people's healthcare steering committee. The research sample was selected using a non-probability, purposive sampling method (Communes were selected based on their socio-economic situation). We built the interview table based on the national criteria setting for commune and ward health for the period up to 2030 with scoring instructions. The interview data collection period was conducted from January to June 2023. This data is not intended to be generalized, but it helps us understand the current state of medical equipment, medical staff, doctors, medical examination and treatment and dispensing medicine to disadvantaged groups in the area. Combining interview results and information from direct discussions with interviewees, we have drawn out the shortcomings and difficulties in building medical facilities in communes and wards according to national standards.
3.3 Quantitative research
In this section, we employed a stratified random sampling method. In each region of Vietnam, we selected two provinces with differences in living conditions and disadvantaged groups. For example: In the mountainous provinces of the Northwest and Northeast, there are many disadvantaged people from ethnic minority groups and the poor. The provinces of the South-Central region and the Red River Delta are socio-economically developed areas, which made it easy to reach target groups such as older adults, gay, bisexual and transgender people. The survey sample size included 4,400 disadvantaged people selected from the list of the social policy department (each province selected 2 communes and wards). The survey was built based on criteria for issuing free health insurance cards, regulations on universal education, multidimensional poverty standards, and social work activities in hospitals. The purpose of collecting primary data was to evaluate the situation of free health insurance cards for disadvantaged groups, medical examination and treatment activities, and the support of social workers local associations and medical facilities. During the survey, we informed the purpose of the study and obtained participants' consent. The survey was supported by local officials and conducted at commune health stations or the homes of disadvantaged people. The survey data collection period was from January to June 2023. The findings from the quantitative and qualitative phases were integrated to formulate recommendations for the Vietnamese government and management agencies.
4 Results
4.1 The current state of health financing and equity in healthcare for disadvantaged people in Vietnam
The Vietnamese government has implemented many policies (in three phases) to support and ensure equity in health care for disadvantaged groups. Phase 1 is about prioritizing policies for health issues that affect vulnerable groups. Phase 2 is policies to increase access to health care services for disadvantaged groups. Phase 3 is financial support policies for disadvantaged groups to access medical examination and treatment.
The Government issued Decision No. 45/HDBT (1989) on collecting medical hospital fees and clearly regulating hospital fee exemptions and reductions for disadvantaged groups such as persons with a disability, orphans, older adults, ethnic minorities living in mountainous areas and children under 6 years old (p.1). In 1995, recognizing the importance of the commune health system in healthcare activities for disadvantaged groups right in the areas where they live, Vietnam issued Decision No. 131/QD-TTG (1995) to strengthen the local medical network. Accordingly, the government used the state budget to pay salaries and allowances for health workers in communes, wards, and villages (p.1). Its achievements have helped significantly improve people's health, especially disadvantaged groups. Next, the government issued Decision No. 75/2009/QD-TTG (2009) to build commune health stations in all communes, eliminate white communes in terms of health, and consolidate and perfect the basic healthcare network facility, which emphasizes ensuring basic healthcare at low cost, contributing to equity in healthcare. This is an important policy on financial resources to support and encourage village health workers, contributing to improving the quality of healthcare, towards equity, efficiency, and development (para.9). In 2013, the government issued Decision No. 122/QD-TTG (2013) approving the "National strategy to protect, care for and improve people's health in the period 2011-2020, with a vision to 2030". The goal of the strategy is to innovate and perfect the Vietnamese health system in the direction of Equity - Efficiency - Development; ensuring all people, especially the poor, ethnic minorities, children under 6 years old, policy beneficiaries, people in disadvantaged areas, remote areas, border areas, islands and other groups of disadvantaged people have access to quality basic healthcare (para.3). This decision also stipulates an increase in the annual budget spending rate for health, ensuring that the growth rate of health spending is higher than the average growth rate of the state budget. It also calls for spending at least 30% of the State's health budget on preventive medicine, ensuring enough funding for regular operations of commune and ward health stations and allowances for village and village health workers, developing appropriate financial mechanisms for primary healthcare activities, prioritizing budget for healthcare of the poor, ethnic minorities, and people in difficult socio-economic areas (para.51). In 2017, Resolution No. 20-NQ/TW (2017) of the 12th Party Central Committee affirmed its commitment to "Building a health system that is equitable, quality, effective and internationally integrated. Develop scientific, ethnic, and mass medicine. Ensuring that all people have healthcare and management” (para.19). After 5 years of implementation of the Resolution, Vietnam has achieved significant improvement in people's healthcare, especially for disadvantaged groups, making an important contribution to the development and building of social security in Vietnam's society.
Vietnam has achieved many positive results through the policies on health financing and creating equity in key healthcare mentioned above. The Ministry of Health (2023) reported on implementing the 2022 Socio-Economic Development Plan according to Resolution No. 32/2021/QH15 of the National Assembly, and the health sector has reached and exceeded 3/3 of the target. The target of doctors per 10,000 people was 11.5, the number of hospital beds per 10,000 people was 31 and health insurance participation rate reached 92.03% of the population (para.8). Vietnam has also implemented a project to invest in facilities, including building 138 new commune and ward medical stations and renovating and upgrading 325 medical stations, renovating, and upgrading 12 district medical centers in 13 provinces from capital sources through aid and loan capital (Ha, 2023, para.4).
Vietnam has built and promulgated a system of legal documents on developing the social work profession, consolidating and developing the network of establishments providing social work services and social work training. Specifically, the government and state management agencies have created a legal corridor to develop the social work profession through legal documents. These documents create conditions for local educational institutions and social work organizations to gradually develop professional social work. The network of social work service providers in localities has developed rapidly. Hoi (2017) reported that Vietnam currently has about 35,000 people working in 418 social protection facilities, more than 100 counseling/consultation centers, and loving homes (para.4). In addition, thousands of part-time social and cultural officers in the community have been forming a network to perform the task of assisting and providing social work services to disadvantaged and disadvantaged groups trauma in the community. Thanh & Dong (2023) quoted the statement of the leader of the Ministry of Health: "The social work network at the hospital is present in most hospitals from the central level to the district levels throughout the country. Social work human resources in hospitals are constantly increasing in quantity and quality” (p.2). The number of social workers at hospitals has expanded from about 500 to more than 6,000, with 1,605 full-time social workers (p.2). The steady increase of social workers in medical examination and treatment facilities shows that the health sector is interested in supporting people and helping people access healthcare services.
4.2 Health financing and equity in healthcare for disadvantaged people in Vietnam
The national criteria for commune and ward health was used to evaluate the effectiveness of medical financial investment and the ability to provide medical examination and treatment services at people's places of residence (Ministry of Health, 2023). The results of the self-assessment of managers of the Commune People's Healthcare Steering Committee on the implementation of the National Criteria for Commune and Ward Health are presented in Table 1.
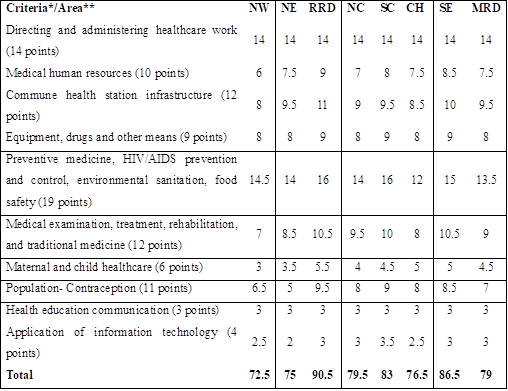
Table 1: Results of self-assessment of implementation of the
National Criteria for Commune Health
*According to No.: 1300/QD-BYT, A national criteria for commune and ward health for up to 2030
**Northwest (NW), Northeast (NE), Red River Delta (RRD), North Central (NC), South Central (SC), Central Highlands (CH), Southeast (SE), Mekong River Delta (MRD)
Source: Compiled survey data by the research team
The self-assessment results of management staff showed that 12 communes met national health criteria out of a total of 32 communes conducting interviews. The criteria that have not been met are listed as follows: Mountainous provinces, with difficult living conditions, make it difficult to attract human resources. Commune health stations often do not have doctors working or have difficulty traveling, so they often arrive late at the announced time. Many areas do not ensure enough rooms and enough area in each room to perform assigned functions and tasks, according to regulations in Circular 32/2021/TT-BYT of the Ministry of Health. Commune and ward health stations lack minimum equipment as prescribed in Circular No. 28/2020/TT-BYT. Many commune and ward health stations do not have enough human resources to access and control screening for early detection of hypertension, people at high risk or suspected of having diabetes due to scattered population density in remote areas. Health management of people in the area, including prenatal check-ups at least four times in 3 periods of pregnancy, is difficult to implement because of problems with the customs and traditions of ethnic minorities. Many children under 1 year old have not been vaccinated with universal vaccines according to regulations of the Ministry of Health.
Table 2. Information on area of residence and health insurance cards of disadvantaged groups
|
Region/Province |
Total respondent |
Free health insurance card |
Voluntary health insurance card |
No health insurance card |
|
Northwest (Lao Cai, Hoa Binh) |
550 |
343 |
130 |
77 |
|
Northeast (Ha Giang, Lang Son) |
471 |
357 |
90 |
24 |
|
Red River Delta (Hanoi, Nam Dinh) |
591 |
222 |
302 |
67 |
|
North Central (Nghe An, Quang Binh) |
639 |
460 |
146 |
33 |
|
South Central (Da Nang, Ninh Thuan) |
577 |
325 |
219 |
33 |
|
Central Highlands (Dak Lak, Gia Lai) |
393 |
297 |
58 |
38 |
|
Southeast (Binh Duong, Tay Ninh) |
661 |
487 |
156 |
18 |
|
Mekong River Delta (Can Tho, Soc Trang) |
518 |
288 |
197 |
33 |
|
Total |
4,400 |
2,779 |
1,298 |
323 |
Source: Compiled survey data by the research team
In this section, we present survey data (except personal information) of the disadvantaged groups participating in the interviews. The living areas of disadvantaged people participating in the survey are in all eight economic regions of Vietnam. Each region selected two economically and socially representative provinces to conduct the survey. The number of people participating in the survey in each area is quite even, on average 550 people/area. Regarding health insurance cards for disadvantaged groups, survey data showed that 2,779 people had health insurance cards issued for free (63.2%), 1,298 people bought health insurance cards (29.5%), the remaining 323 people did not have health insurance cards (7.3%). This survey data resonates with the Ministry of Health's Report (2022) on the health insurance coverage rate in Vietnam of 92.04%. In the survey, a high proportion of the disadvantaged subjects have to buy health insurance by themselves. The reason is that some disadvantaged people in Vietnam are not granted free health insurance cards, such as gay, bisexual, transgender people, older adults between the ages of 70 and 79, and some poor people.
Table 3. Survey results on disadvantaged groups, education level and household economy
Unit: Person
|
Criteria/Area* |
NW |
NE |
RRD |
NC |
SC |
CH |
SE |
MRD |
Total |
|
Disadvantaged groups |
|||||||||
|
Ethnic minority |
378 |
316 |
42 |
256 |
280 |
322 |
215 |
267 |
2,076 |
|
Elderly |
43 |
23 |
124 |
39 |
17 |
26 |
55 |
33 |
360 |
|
Poor |
242 |
218 |
106 |
147 |
119 |
232 |
127 |
168 |
1,359 |
|
People with disabilities |
14 |
11 |
125 |
122 |
24 |
66 |
51 |
23 |
436 |
|
People infected with HIV/AIDS |
8 |
5 |
89 |
11 |
37 |
14 |
36 |
28 |
228 |
|
Gay, bisexual, transgender |
4 |
7 |
63 |
19 |
6 |
2 |
16 |
2 |
119 |
|
Children |
33 |
25 |
59 |
26 |
14 |
18 |
29 |
44 |
248 |
|
Academic level** |
|
|
|
|
|
|
|
|
|
|
Unlettered |
171 |
115 |
0 |
12 |
5 |
37 |
3 |
19 |
362 |
|
Are literate |
371 |
334 |
446 |
551 |
533 |
303 |
566 |
467 |
3,571 |
|
Have professional qualifications |
8 |
22 |
145 |
76 |
39 |
53 |
92 |
32 |
467 |
|
Household economy*** |
|
|
|
|
|
|
|
|
|
|
Poor household standard |
242 |
218 |
106 |
147 |
119 |
232 |
127 |
168 |
1,359 |
|
Near-poor household standards |
302 |
245 |
314 |
363 |
352 |
91 |
392 |
264 |
2,323 |
|
Standard household has an average standard of living |
6 |
8 |
120 |
88 |
78 |
56 |
105 |
82 |
543 |
|
Other |
0 |
0 |
51 |
41 |
28 |
14 |
37 |
4 |
175 |
*Northwest (NW), Northeast (NE), Red River Delta (RRD), North Central (NC), South Central (SC), Central Highlands (CH), Southeast (SE), Mekong River Delta (MRD)
** According to Decree No. 20/2014/ND-CP on universal education, literacy and Education Law No. 43/2019/QH14, children are assessed through their guardians.
***According to Decree No. 07/2021/ND-CP, Regulations on multidimensional poverty standards for the period 2021 – 2025
Source: Compiled survey data by the research team
According to information from VSS (2017), the group classified as disadvantaged workers in Vietnam has about 13 million people (para.1). Table 3 summarises the number of disadvantaged groups in the research area, education level and household economy. Ethnic minorities are the disadvantaged group with the highest proportion with 2,076 people. Specifically, in the Northeast region, the main ethnic minorities are Tho, La Chi, Tay, Dao, Man, Nung, and San Chay. The Northwest region has ethnic minorities such as Mong, Dao, and Muong. The Red River Delta region has ethnic minorities such as Muong, Dao, and San Diu. The North Central region has ethnic minorities such as Thai, Tho, Kho Mu, Mong, and O Du. The south-central region has Hre, Co Ho, Xo Dang, Cham, Ba Na, E De, Ra Glai, Gie Trieng. The Central Highlands has Gia Rai, E De, and Ba Na. The Southeast has Hoa, Nung, Cho Ro, Muong, Khmer, Ma, and S'tieng. The Mekong River Delta has Cham, Khmer and Chinese. The poor group has the second largest number with 1,359 people, mainly distributed in mountainous areas and the Central Highlands, with difficult economic conditions. The group of elderly people and people infected with HIV/AIDS are mainly concentrated in areas with more developed economic conditions such as the Red River Delta, North Central, and Southeast. The remaining disadvantaged groups account for a smaller proportion and are distributed quite evenly across regions. One point worth noting is that many disadvantaged people are both ethnic minorities and poor people. These objects often appear in mountainous, remote, and mountainous areas.
The educational level of disadvantaged people is assessed according to three levels: illiterate, literate and professionally qualified. The group of disadvantaged people who are literate is 3,571 people (81%). The group with professional level has the second highest proportion/hold the second position at 10.6% (with 3,517 people). Finally, there is the disadvantaged group, which is illiterate. This group faces many difficulties in daily life, including difficulties in accessing social services and inequity in healthcare. They are often disadvantaged people from ethnic minorities, living in remote mountainous areas far away from local social organizations.
Household economics in the survey were collected according to Vietnam's multidimensional poverty standards, including poor households, near-poor households, and households with an average living standard. Disadvantaged people often have difficulty finding work. They mainly engage in seasonal work, farming, and animal husbandry, resulting in lower incomes. Only a few disadvantaged people with professional qualifications can find jobs and have stable living and economic conditions. The near-poor group accounts for the largest number with 2,323 people, mainly gay, bisexual, transgender, and some ethnic minorities. The Poor Households Group has 1,359 people, mainly ethnic minorities, people living with HIV, the elderly, and people with disabilities, which is a very large difference compared to other developed economic regions of Vietnam.
These survey data are common indicators used to assess equity in healthcare. These numbers explain the barriers and difficulties that disadvantaged people face in accessing medical examination and treatment services, including those who have free health insurance cards.
Figure 1. Results of data analysis on disadvantaged people who have not had medical examination and treatment in 3 years (2020-2022)
Unit: %
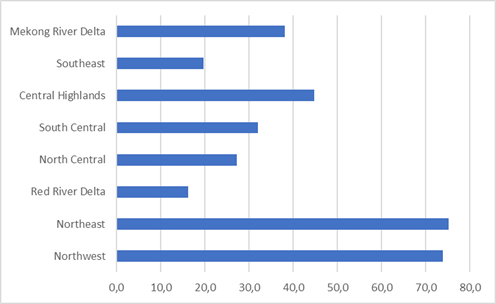
Source: Analysis of survey data by the research team
In the northern mountainous regions of the Northeast and Northwest, the rate of people not using healthcare services was nearly 80%, calculated based on the number of survey participants in each region. This is a number that goes against the goal of "Ensuring that all people have healthcare and management" stated in Resolution No. 20-NQ/TW on strengthening the protection, care, and improvement of Vietnam people's health. The regions with the lowest rate of disadvantaged people not having medical examination and treatment in 3 years are the Red River Delta at 16.2%, the Southeast at 19.7%, and the North Central region at 27.2%. We assessed the reasons why they did not have regular medical examinations and treatment through a group of closed survey questions. This group of questions only surveys people who do not take care of their health. Data analysis results show that the factor of high costs paid for medical examination and treatment services was agreed by 1,321 people (76.9%). In Vietnam, some medical diagnostic techniques and drug lists for dangerous diseases are not covered by health insurance, so people must pay part of the costs from their own pockets. Hoang (2023) while observing the high out-of-pocket expenditure, stated that "costs paid for medical examination and treatment services from the out-of-pocket cost of health service users is still at 43%, quite high compared to many countries in the world and the WHO recommendation is 20%” (p.1). The poor and near-poor often do not use medical examination and treatment services because they cannot afford to pay. Two factors "The feeling of inferiority complex, fear of social barriers" and "Ineffective medical examination and treatment" have the second largest influence with 66.6% and 58.7%. The remaining factors all influence over 50% of disadvantaged people's intention to access medical examination and treatment services.
Table 4. Analysis results of factors affecting the use of medical examination and treatment services
|
Factor |
Yes |
No |
||
|
Frequency |
% |
Frequency |
% |
|
|
The cost of medical examination and treatment services is high |
1,321 |
76.9 |
397 |
23.1 |
|
Feeling of inferiority complex, fear of social barriers |
1,010 |
58.7 |
708 |
41.3 |
|
Medical treatment is not effective |
1,145 |
66.6 |
573 |
33.4 |
|
Customs and traditions, worship of gods |
918 |
53.4 |
800 |
46.6 |
|
Lack of information about medical examination and treatment policies for disadvantaged people |
746 |
43.4 |
972 |
56.6 |
Source: Analysis of survey data by the research team
To evaluate the effectiveness of local social work activities, we surveyed disadvantaged groups who did not have access to health care services. The results in Table 5 show that, out of more than 1,700 people whose opinions were polled, 156 people (9.1%) received psychological counseling and support from social workers to overcome their inferiority complex. The number of people who was encouraged by social workers for medical examination and treatment and regular health check-ups was 107 people (6.2%). The low effectiveness of social work activities is due to the shortage of social workers in Vietnam. Social work profession is not highly appreciated and has not received proper attention, especially in regional areas, mountains, and remote areas. The results in Table 5 also show positive data on the number of people receiving advice on medical examination and treatment policies using health insurance cards and government medical support policies (rate of 25%). This result is due to the support from the Vietnam Social Insurance Agency in communicating health insurance policies to the people according to Resolution No. 96/NQ-BCS.
Table 5. Analysis results of support measures of social workers at home
|
Criteria |
Yes |
No |
||
|
Frequency |
% |
Frequency |
% |
|
|
Receive psychological counseling and support from social workers |
156 |
9.1 |
1,562 |
90.9 |
|
Encouraged by social workers to carry out medical examinations and treatment and have regular health checks |
107 |
6.2 |
1,611 |
93.8 |
|
Get advice from social workers on medical examination and treatment policies using health insurance cards and government medical support policies |
429 |
25.0 |
1,289 |
75.0 |
Source: Analysis of survey data by the research team
In the final phase of the quantitative research, we evaluated the support activities of social workers at the hospital. Disadvantaged people who use medical examination and treatment services answered these questions. The survey results are presented in Table 6. Specifically, 597 people (22.7%) received support and advice from hospital social workers to solve problems during medical examinations and treatment. Several 1,091 people (41.5%) said they received support but lacked enthusiasm. Not receiving consulting support to solve problems during medical examination and treatment from social workers was reported by 944 people (35.9%). On being asked if social workers provided information about policies and patient rights 241 people (9.2%) said "Yes, enthusiastically", 975 people said there was support but a lack of enthusiasm, and 1,416 people (53.8%) did not receive any information in this regard. When inquired if social workers were helpful in addressing psychological problems such as stress and depression, creating confidence in the treatment process 112 people (4.3%) were talked to and listened to by hospital social workers, 558 people (21.2%) thought that the support from social workers lacked enthusiasm and 1,962 people (74.5%) did not receive support. In the last question, only 27 people (1%) received enthusiastic support from social workers when calling for and mobilizing funding for medical examination and treatment costs within 3 years.
Table 6. Results of survey data analysis on support activities of hospital social workers
|
Criteria |
Yes, enthusiastically |
Yes, not enthusiastic |
No |
|||
|
Frequency |
% |
Frequency |
% |
Frequency |
% |
|
|
Get support and advice from hospital social workers to solve problems during medical examination and treatment |
597 |
22,7 |
1,091 |
41,5 |
944 |
35,9 |
|
Be provided with information by hospital social workers about policies and patient rights in medical examination and treatment |
241 |
9.2 |
975 |
37.0 |
1,416 |
53.8 |
|
Have hospital social workers talk to you and listen to you share about psychological problems such as stress and depression, creating confidence in the treatment process. |
112 |
4.3 |
558 |
21.2 |
1,962 |
74.5 |
|
Called and mobilized by hospital social workers to sponsor medical examination and treatment costs |
27 |
1.0 |
121 |
4.6 |
2,484 |
94.4 |
Source: Analysis of survey data by the research team
From the survey analysis results, we found that the number of disadvantaged people who did not receive support from social workers at the hospital was very high, on average nearly 70%. The reason is that the implementation of the social work profession development project No. 32/2010/QD-TTg was quite slow, issued in 2010 but not implemented until 2015 through Circular No. 43/2015/TT-BYT laying down regulations on tasks and forms of organization to perform social work tasks in hospitals. Slow implementation is the reason why the scale of social work in hospitals is slow to develop. The social work network in hospitals has only been deployed at central, provincial and district medical examination and treatment facilities. Therefore, disadvantaged people who receive medical examinations and treatment at the commune and ward health stations will not receive support from social workers. Vietnam has nearly 60 universities that train social workers, but only the University of Public Health is a school that trains social workers in hospitals. Most social workers have not been properly trained and nurtured in knowledge and skills, so they lack professionalism, and their performance is not as expected. This is also one of the reasons why disadvantaged people receive support but not enthusiastically from social workers. In addition, disadvantaged groups have the characteristic that they only go for medical examination and treatment when they are seriously ill, especially people with disabilities, older adults, and people with HIV/AIDS. They need support for physical, mental and psychological care and treatment. However, due to a lack of social workers and/or social workers lacking professional qualifications, helping patients effectively through social work interventions is difficult.
5 Policy Implications
5.1 Government
Specific regulations for subjects belonging to disadvantaged groups: Currently, disadvantaged people in Vietnam are regulated scatteredly in many legal documents. Some disadvantaged people have difficulties in daily life and health but do not receive timely access and support. Therefore, the state needs to issue detailed regulations on disadvantaged groups. Accurately defining target groups will help deploy medical support and social work support faster and simpler.
Developing the grassroots healthcare system, especially commune and ward healthcare, to attract human resources: To create conditions for disadvantaged groups to easily access health services, meet medical examination and treatment needs and reduce costs, Vietnam needs to increase health investment funding, quickly promote socialization, and develop the public health system. Improving the quantity and quality of staff at the commune and ward health stations is also required.
Innovating the health financing mechanism to ensure financial support for healthcare for disadvantaged people: To increase support for medical examination and treatment costs and to reduce payments for medical services from people's own money, the financial system must receive more support from the Government and social organizations.
Promote the implementation of Circular No. 43/2015/TT-BYT on organizing the implementation of social work tasks in hospitals: Adding social workers to medical examination and treatment facilities in local and remote areas is an essential step. Ensuring that each commune, ward, and town has at least 5 commune workers can help in ensuring prompt support to disadvantaged people.
Continue to improve the institutional and legal system: This ensures the legal corridor for social work activities and development such as the Labor Code, Law on Protection, Care and Education of Children, Code of Conduct Civil Law, Law on Domestic Violence Prevention and Control, and Gender Equality Law.
5.2 Training
Increasing the responsibility of educational agencies and local management agencies to propagate and raise awareness of disadvantaged groups about illiteracy eradication is essential. Innovating management, investigation, advocacy, and organization of illiteracy eradication classes can be helpful. Creating coordination between educational institutions and local social workers in implementing illiteracy eradication work can improve the status of the disadvantaged groups. Improving the quality of teaching and learning in illiteracy eradication programs; supplementing regimes and policies for disadvantaged people when participating in learning etc. can also be helpful in this regard.
The Ministry of Labor, Invalids and Social Affairs coordinates with higher education institutions to develop social work training programs according to standards and quality assurance. Completing the plan to develop social work education and training for bachelor's degrees at universities, colleges, and vocational training establishments with specialized training in health social work can be instrumental in this aspect.
5.3 Medical facilities
Developing a roadmap for organizing the Social Work Department in the hospital according to the provisions of Circular 43 is one of the necessary steps in improving health social work practice in Vietnam. This will help improve the training and quality of social workers in hospital settings. This can also attract students and boost social work training in Vietnam. The curriculum must include content to improve social work skills and orientation on special healthcare consulting support for persons with disability and older adults
There is also a need to increase awareness and interest of hospital heads in directing and properly implementing social work tasks at hospitals according to regulations of the Ministry of Health, contributing to care and protection and improving people's health.
5.4 Social work organizations
On the part of social work organizations, it is necessary to train and build a team of social work staff to ensure that human resources operate and directly approach disadvantaged people to support and advise them on solving psychological and legal problems.
Vietnamese social organizations need to increase their influence, call for non-governmental aid sources, and aid from social organizations worldwide to supplement Vietnam's health financial resources, contributing to opening and expanding free medical services for serious illness groups.
Social workers at medical examination and treatment facilities need to call for community activities from groups of young doctors, forming medical volunteer groups operating in economically difficult areas.
6 Conclusion
To increase equity and efficiency in medical care, Vietnam needs solutions from both sides: state agencies and social work organizations. On the government side, Vietnam needs to continue to expand health insurance coverage for disadvantaged groups social work professionals should advocate for improving the quality of medical service provision, especially at grassroots medical levels, remote areas, with more modern medical examination and treatment equipment, and attract a team of qualified medical staff so that disadvantaged people can receive effective treatment right in their living areas. As for social work organizations, it is necessary to focus on training and building a team of social work staff to ensure human resources operate and add to the social work network of the whole country. Social workers should engage with disadvantaged people to provide them with psychological and legal advice. Social workers shall also mobilize human and financial support from aid sources to increase the affordability of the health financing system. In addition, management agencies need to coordinate with social work organizations to propagate and change the awareness, attitudes, and behaviors of disadvantaged groups so that they can understand the benefits and procedures, medical examination, and treatment procedures to use health insurance cards more effectively.
Limitations of the study: The research has accomplished the set goals, but it also has a limitation in that we have not reached and surveyed disadvantaged people living on Vietnam's islands.
Acknowledgement: This research is of the outcome of the project: "Research on the possibility of implementing supplementary health insurance in Vietnam". Code: B2023.KHA.05
Conflict of Interest: The authors reported no potential conflict of interest.
References:
Bac, H. T. (2023). Effectively ensure access to information for disadvantaged groups in society. Electronic Toa An Nhan Dan Magazine. Accessed on June 5, 2023, from https://tapchitoaan.vn/bao-dam-hieu-qua-quyen-tiep-can-thong-tin-cua-nhom-doi-tuong-yeu-the-trong-xa-hoi8649.html
Communist Party of Vietnam. (2011). Documents of the 11th National Congress. National Politics, Hanoi, pp.128 – 129
Communist Party of Vietnam. (2017). The sixth conference of the Central Executive Committee, term XII, on strengthening the work of protecting, caring for and improving people's health in the new situation. Number: 20-NQ/TW. Accessed on December 5, 2022, from https://thuvienphapluat.vn/van-ban/The-thao-Y-te/Nghi-quyet-20-NQ-TW-2017-tang-cuong-cong-tac-bao -ve-cham-soc-nang-cao-suc-show-nhan-dan-365599.aspx
Council of Ministers. (1989). Decision on collection of part of medical hospital fees. No: 45/HDBT. Accessed on December 8, 2022, from https://thuvienphapluat.vn/van-ban/Thue-Phi-Le-Phi/Quyet-dinh-45-HDBT-thu-mot-phan-vien-phi-y-te -37751.aspx
Cuong, D. V. (2005). Towards implementing fairness in people's healthcare: Problems and solutions, Publishing House. National Politics, Hanoi, p.32
Chuc, N. T. K. (2007). Health economics and health insurance, Medical Publishing House, Hanoi, Vietnam
Dung, V. (2021). Social adaptation of such social groups in our country today. Institute of Psychology, Encyclopedia.
Evin, C. (2003). Equity and financing of the health sector in transition countries. Workshop "For a growth and equitable society" - Ho Chi Minh City September 10-11, 2003
Gapenski, L. C., & Reiter, K. L. (2012). Healthcare finance: An introduction to accounting and financial management. Chicago, Illinois: Healthcare Management Press.
General Statistics Office. (2022). Statistical Yearbook 2022. General Statistics Office, Vietnam
Government. (2014). Decree on universalization of education and eradication of illiteracy. No: 20/2014/ND-CP. Accessed November 13, 2022, from https://vanban.chinhphu.vn/default.aspx?pageid=27160&docid=172926
Government. (2021). Decree regulating multidimensional poverty standards for the period 2021 - 2025. No.: 07/2021/ND-CP. Accessed on December 8, 2022, from https://vanban.chinhphu.vn/?
Ha, T. (2023). Invest 126 million USD for the basic health system. Government Electronic Newspaper. Accessed September 28, 2023, from https://baochinhphu.vn/dau-tu-126-trieu-usd-cho-he-thong-y-te-co-so-102278079.htm
Hai, N.N. (2016). Financial policy for public health development in the market economy in Vietnam. Doctoral thesis in economics, University of Economics and Law
Hoang, M. (2023). 43% of medical examination and treatment costs come from the pocket of health service users, Nhan Dan Newspaper, accessed July 29, 2023, from https://nhandan.vn/43-chi-phi-kham-chua- health-la-tu-tien-tui-cua-nguoi-su-dung-dich-vu-y-te-post641088.html
Hoi, N. V. (2017). Results of 6 years of implementing the Project on developing the social work profession and tasks in the coming period. Journal of Labor and Society. Accessed on December 8, 2022, from https://tapchilaodongxahoi.vn/ket-qua-6-nam-thuc-hien-de-an-phat-trien-nghe-cong-tac-xa-hoi-va-nhiem-vu-giai-doan-toi-1305750.html
Ministry of Health. (2008). General report on health sector overview 2008, Health Finance in Vietnam. Retrieved March 20, 2023, from https://cphs.huph.edu.vn/uploads/tainguyen/sachvabaocao/JAHR2008(Vn).pdf
Ministry of Health. (2015). The Circular regulates the tasks and forms of organizing the implementation of social work tasks of hospitals. No: 43/2015/TT-BYT. Accessed on November 22, 2022, from, https://thuvienphapluat.vn/van-ban/The-thao-Y-te/Thong-tu-43-2015-TT-BYT-hinh-thuc-to-chuc-thuc-hien -nhiem-vu-cong-xa-hoi-cua-Benh-vien-296470.aspx
Ministry of Health. (2020). The Circular regulates the list of minimum equipment for commune-level medical stations. Number: 28/2020/TT-BYT. Accessed on December 20, 2022, from https://luatvietnam.vn/y-te/thong-tu-28-2020-trang-thiet-bi-toi-thieu-cua-tram-y-te-tuyen-xa -196451-d1.html
Ministry of Health. (2021). Circular Promulgating Guidelines for basic design of commune, ward and town health stations. No: 32/2021/TT-BYT. Accessed on December 20, 2022, from https://luatvietnam.vn/y-te/thong-tu-32-2021-tt-byt-215147-d1.html.
Ministry of Health. (2023). Decision to promulgate a set of national criteria for commune and ward health for the period up to 2030. No.: 1300/QD-BYT. Accessed on April 5, 2023, from https://thuvienphapluat.vn/van-ban/The-thao-Y-te/Quyet-dinh-1300-QD-BYT-2023-Bo-tieu-chi-quoc-gia -ve-y-te-xa-den-2030-558680.aspx
Ministry of Health. (2023). Health insurance coverage reached 92.04%: Humane and meaningful security policies are increasingly multiplied. Hanoi, Retrieved August,18.2023, from https://moh.gov.vn/tin-lien-quan/-/asset_publisher/vjYyM7O9aWnX/content/bao-phu-healthinsurance-at-92-04-chinh-sach- an-sinh-nhan-van-y-nghia-ngay-cang-uoc-nhan-len
Ministry of Health. (2023). Report on implementation of the 2022 Socio-Economic Development Plan. Accessed on February 26, 2023, from https://moh.gov.vn/home?p_p_id=101&p_p_lifecycle=0&p_p_state=maximized&p_p_mode=view&_101_struts_action=%2Fasset_publisher%2Fview_content&_101_type =content&_101_urlTitle=nam-2022-nganh-y-te-a-vuot-and-at-ca-3-chi-tieu
Ministry of Health. (n.d.). Health policy component project: Health financial solutions for the poor, Medical Publishing House, Hanoi, pp. 12 - 13
Ministry of Health. (n.d.): Index for monitoring and evaluating equity and efficiency in healthcare, Ministry of Health, pp. 6 - 9
National Assembly. (2014). Law amending and supplementing several articles of the health insurance law. No.: 46/2014/QH13, Office of the National Assembly, Vietnam
National Assembly. (2019). Education law. Law No.: 43/2019/QH14. Accessed on December 8, 2022, from https://vanban.chinhphu.vn/default.aspx?pageid=27160&docid=197310.
Prime Minister. (1995). Decision to amend a number of points in Decision 58/ttg dated February 3, 1994, on organization and policies for grassroots healthcare. Number: 131-TTg. Accessed on December 8, 2022, from https://thuvienphapluat.vn/van-ban/The-thao-Y-te/Quyet-dinh-131-TTG-to-chuc-che-do-chinh-sach-y -te-co-so-sua-doi-Quyet-dinh-so-58-TTg-39082.aspx
Prime Minister. (2009). Regarding regulations on allowances for village health workers. No: 75/2009/QD-TTg. Accessed on December 9, 2022, from https://chinhphu.vn/default.aspx?pageid=27160&docid=86742.
Prime Minister. (2010). Decision approving the project to develop the social work profession for the period 2010 - 2020. No.: 32/2010/QD-TTg. Accessed September 28, 2023, from https://thuvienphapluat.vn/van-ban/Van-hoa-Xa-hoi/Quyet-dinh-32-2010-QD-TTg-phe-duyet-De-an-phat -trien-listening-cong-tac-xa-hoi-giai-doan-2010-2020-102910.aspx
Prime Minister. (2013). Decision Approving the National Strategy to protect, care for and improve people's health for the period 2011 - 2020, with a vision to 2030. No.: 122/QD-TTg. Accessed on December 9, 2022, from https://chinhphu.vn/default.aspx?pageid=27160&docid=165437.
Quy, T. T. T. (2015). Equity in healthcare in Vietnam today. Dan Van Magazine. Accessed on February 28, 2023, from http://danvan.vn/Home/Nganh-y-te-voi-cong-tac-dan-van/1628/Cong-bang-trong-cham-soc-suc-khoe-o-Viet-Nam-hien-nay
Quyen, A. (2019). Need to pay more attention to disadvantaged groups in society, Economy & Forecast Review. Retrieved September 20, 2023, from https://kinhtevadubao.vn/can-quan-tam-nhieu-hon-toi-nhom-yeu-the-trong-xa-hoi-10939.html
Quyet, P. V., & Tuan, P. A. (n.d.). Support work for disadvantaged groups in Vietnam. Accessed February 5, 2023, from https://congtacxahoi.com.vn/cong-tac-ho-tro-nhom-yeu-o-viet-nam/.
Thanh, T., & Dong, V. (2023). Social work in health contributes positively to comprehensive patient care, Health and Life Magazine. Accessed September 22, 2023, from https://suckhoedoisong.vn/cong-tac-xa-hoi-trong-y-te-dong-gop-tich-cuc-cho-viec-cham-soc-toan-dien -nguoi-benh-169230729154458273.htm#:~:text=T%E1%BB%AB%20kho%E1%BA%A3ng%20500%20ng%C6%B0%E1%BB%9Di%20l%C3%A0m, h%C3%A0i%20l%C3%B2ng%20c%E1%BB%A7a%20b%E1%BB%87nh%20nh%C3%A2n.
Vietnam Social Security. (2017). Find sustainable livelihood solutions for disadvantaged labor groups in Vietnam. Hanoi, Retrieved August,10.2023, from https://baohiemxahoi.gov.vn/gioithieu/Pages/gioi-thieu-chung.aspx?CateID=0&ItemID=9160.
Vu, A. D. (2013). Measuring the quality of healthcare services. Department of Quality Management, Ministry of Health.
World Health Organization. (n.d.). Vietnam health finance. Accessed March 22, 2023, from https://www.who.int/vietnam/vi/health-topics/health-financing.
Author´s
Address:
Thi Xuan Huong Le
Ph.D. University of Labour and Social Affairs, Vietnam
+84938687686
lexuanhuong.ins@gmail.com
Author´s
Address:
Thi Hai Duong Nguyen
Ph.D. National Economics University, Vietnam
+84935918918
duongnh.neu@gmail.com
https://orcid.org/0000-0003-4098-3550
Author´s
Address:
Thi Thuy Dung Nguyen
MSc.MD. Military Hospital 103, Vietnam
+84977815585
Bsdunga12@gmail.com
Author´s
Address:
Thi Huu Ai Nguyen
Ph.D. University of Labour and Social Affairs, Vietnam
+84353355188
nguyenhuuai.ins@gmail.com
Author´s
Address:
Thi Huong Tram Le
MSc. University of Labour and Social Affairs, Vietnam
+84978500250
huongtramle@gmail.com
Author´s
Address:
Nguyen Zen Nguyen
MA. University of Labour and Social Affairs, Vietnam
Zennguyen89@gmail.com
https://orcid.org/0009-0004-6878-4005