Suppressed voices and lost opportunities in education and the psychiatric healthcare system – a structural analysis of dilemmas in inter-professional collaboration between sectors
Anne Morin, Aarhus University
“A young person comes in and we may sow a seed but then we meet a municipality that says: Well, they just need to feel a bit better first. This is frustrating because you know that this young person will go back home and sit in front of the computer once again without getting any help for six months. Then they are lost. It doesn’t make sense for such young people. The seed that we sow will only grow if children get the right services, even if it is expensive”. (Psychiatrist, child psychiatric centre)
Despite many years of efforts and initiatives focusing on inclusion and the prevention of poor well-being and exclusion in a national Danish context, there has been an increase in the number of children and young people experiencing mental health problems and not thriving in recent years. Over the past ten years in Denmark, there has been an increase in the number of 0-17 year-olds with registered mental illnesses of more than 50 per cent (The Ministry of Interior and Housing’s Benchmarking Unit, 2020). Childcare centres, schools and child psychiatry services are also experiencing an increase in the number of referrals of children needing to be assessed for possible developmental disorders and diagnoses (Holstein et al. 2021). The trend is also reflected in key figures from the Danish municipalities (KL) for the socially disadvantaged, which in 2019 show that a significant proportion of this group of children have complex problems that can be observed in an increasing proportion of children in childcare institutions and schools. As the research suggests, this situation calls for initiatives aimed at this group of children and young people. These initiatives need to start early, and they also need to be informed by inter-professional collaboration due to the complexity of the problems at hand (Hartnell 2010; Moola & Lazarus 2014; Maki 2019; Law & Woods 2019). In a national Danish context, interventions related to children in difficulties generally include inter-professional processes and forms of collaboration, making it possible to deal with the complexity of the issues involved in connection with investigations and possible interventions. At the political level in Denmark, it is now a defined goal to develop more holistic and earlier efforts through inter-professional and cross-sectoral collaboration, and a number of different models for collaboration between psychiatrists, schools, educational psychologists and municipal departments were launched in January 2019 (Danish Health and Medicines Authority 2018). At the same time, research shows that there are a number of challenges associated with inter-professional collaboration. Research has revealed that individualistic problem understandings where the problem is seen as originating in individual dispositions in the child support processes in which intervention procedures with regard to individual problem determination leads to problem displacement out of the general environment (Hjørne & Säljø, 2014; Hamre et al. 2018). Furthermore, research shows organisational challenges for instance that a lack of coordination between sectors (for instance between the school sector and the health sector or between regions and municipalities) increases the risk that children and families will not receive help in time, and that resources will be wasted (Shahidullah, 2019; Bradley-Klug & Armstrong, 2014; Spiers 2013). Thus, one of the fundamental challenges in relation to the prevention of poor well-being and exclusion is that the contextual everyday knowledge which the professionals in for instance the school possesses is not always sufficiently brought into play before a case is referred to the psychiatric services for examination. At the same time, children and families often have to wait a long time for resources to be allocated, with the risk of further complications and a worsening of the situation facing children and families. This complicates access to resources as well as opportunities to anchor intervention efforts in the everyday school setting (Shahidullah, 2019; Moola & Lazarus, 2014). The article will discuss some of the structural reasons for these dilemmas focusing on organizational challenges in the inter-professional everyday practice resulting in difficulties and lost opportunities in providing timely help and resources for children and families. This discussion will be based on research findings from a development project which I had the opportunity to follow. The study context is presented below.
1 Study context
In the period 2018-21, in a national Danish context, government funds were set aside for trials with various forms of advanced regional functions in a collaboration between psychiatrists, schools and municipalities (Government 2017; Danish Health Agency 2018). The empirical material presented in this article originates in a collaborative research project[1] focusing on the government-financed development project entitled “Strengthened early intervention for children and young people who experience mental health problems and failure to thrive” (Ministry of Health 2018). The aim of this project is to develop and test a model for a coordinated professional joint collaboration to work towards a holistic and cross-sectoral effort in which children and young people can be helped in the least invasive way without involving the psychiatric system and with a view to promoting their well-being. The main goals of the project are: 1) To ensure early detection of children and young people with significant psychological distress. 2) To upgrade professional staff in the early detection and assessment of children/young people with significant psychological distress. And 3) To offer the right interventions for children/young people. In the project new workflows are developed for inter-professional collaboration between key staff in the Danish regions such as social workers, outpatient clinics, doctors and nurses as well as in municipalities in school psychology and in family departments. The project is based on competence development through joint workshops, and is steered by project leaders who are academic employees, based in child psychiatry in collaboration with the steering group of the development project consisting of regional leaders of school psychologists and psychiatrists from the regions and municipalities. In the workshops facilitated by the project leaders, the parties have the opportunity to discuss possibilities and dilemmas relating to collaboration between different sectors. In addition, new procedures for concrete cooperation are tested, for instance new communication channels between the sectors. In my research I have had the opportunity to follow this work by carrying out empirical observations of these workshops and interviews with key participants in a collaborative research endeavour. My main focus in researching the development project is to develop new knowledge about the changes this work with new collaborative cross-cutting professional organizations entails, partly in relation to children’s well-being and development, and partly in relation to the meaning and potential of such changes in relation to the professionals involved and the way they perform their tasks, as well as their professional identity. In other words, my research project has two points of interest: Firstly, based on the concrete development work, to explore selected new forms of organisation related to inter-professional and cross-sectoral collaboration; and secondly, with this point of departure more generally to develop knowledge about professions in processes of organisational change and transition.
In my research I follow selected developmental arenas focusing on for instance the developing of a common cross-sectoral action plan to be implemented in the inter-professional collaboration and development of common competence development across professions. In this way, knowledge is created of opportunities and dilemmas related to development across professions and sectors. Methodologically, the research is conducted in a collaborative practice research tradition. In collaborative practice-based research, local agents develop insights and actions based on knowledge directly from their own practice. As in other kinds of action research (Whyte, 1991), there is often a goal of changing and improving practice in social systems, although this does not have to be the case. Practice research in the Danish-German tradition (Mørch & Hunniche, 2006), which forms the methodological basis of the empirical work in this project, often begins with discussions between researchers and practitioners, but it does not have to end up in an intervention or action agenda. However, the common goal is to bridge the traditional gap between research and practice. Rather than being a fixed method, practice-based research can be seen as evolving from certain ways of organising research (Højholt, 2005). In the Danish-German tradition, practice research as a dialectical theoretical understanding of how people live and develop in the world has had important methodological implications, as seen in the development of the notion of collaboration with co-researchers. The empirical data resulted from observations conducted at workshops, in large forums in which many different professions participated, including school psychologists, psychiatrists, social workers and educators. The aim at the workshops were to create dialogue and to share knowledge among the different professionals and sectors. Additionally, interviews are conducted with key professionals involved in the project as child psychiatrists, educational psychologists and social workers. The empirical data included in this article focuses on parts of interviews, which relate to the question of how structural dilemmas may result in dilemmas and lost opportunities in early inter-professional and cross-sectoral interventions. Having presented the methodological and empirical framework of analysis, I will now present some main dilemmas based on the empirical findings, focusing on inter-professional collaboration and organisational divisions and the fact that divisions between professions may limit opportunities to work holistically and provide timely help for children and families.
2 Inter-professional collaboration, social practice and situated inequality
As mentioned above, inter-professional collaboration, across different sectors is part of task solution and professional decision-making processes in educational and other welfare institutions. This mark a significant and potentially defining shift in the conditions and demarcations of the professional’s tasks, suggesting a move away from profession-centred practice, which links, to a classic expert role, characterized by a high degree of power to define and decide and a fixed division of tasks. Towards a collaborative expertise, which links expertise to action in everyday life's often changing work practices (Engeström, 2018). For a number of years, research has pointed out how divisions between professions limit opportunities to work holistically and create coherence in professional collaboration regarding initiatives aimed at children in difficulty (Edwards 2011; Hjörne & Säljø 2014, 2017; Højholt 2011; Morin 2018). In this research, it is pointed out that inter-professional collaboration creates the opportunity for joint exploration and discussion of given problems and coordination, but may also lead to division, conflict and dysfunctionality (Røn Larsen 2012; Morin 2011). The question of organisational and professional divisions and how divisions between professions may limit opportunities to work holistically and provide timely help is also central in the empirical findings of the research project. At a meeting in one of the municipalities participating in the development project I was as part of my research observing at a resource meeting. The following is from my notes from this meeting:
“A teacher has booked time to present what she feels are serious problems facing one of her students, a sixth-grade boy who we will refer to as Isaac. The teacher describes Isaac as highly unfocused. He has externalising behaviour problems and has tried to strangle another boy from the class. He has also threatened to jump out in front of a train, and the authorities have been notified of his case. At the school the inclusion consultant has been in contact with Isaac and Isaac’s family. She reports that the family are extremely stressed because Isaac’s big brother is violent. The parents are very frustrated and do not have many resources, as explained by the inclusion consultant.
School social worker: I am wondering if Isaac’s father is violent towards the children.
Teacher: Isaac sent me an SMS: I will be beaten up when I get home. My father will throw me to the floor.
School social-worker: The citizens’ advice service should be informed of this. Have they been given this information?
Teacher: I don’t know. I think perhaps long time ago.
School social-worker: They need to be updated, then. Often one professional doesn’t know what other professionals are doing. One idea could be to arrange a meeting with their social worker and perhaps see if we can work in the same direction?
Healthcare professional: Do they get the information from us at the civic centre? Nobody answers.”
This observation raises questions about structural dilemmas and professional access to knowledge, as well as indicating the presence of organisational dilemmas, which may complicate a coordinated and timely intervention plan. As specific professional locations and positions include specific opportunities, limitations and disposal for the person from each specific location and position persons have different opportunities of access to knowledge. As the empirical example above reveals, professionals who collaborate in dealing with children who are experiencing difficulties have different social practices, and so they inhabit different positions. For instance, they carry out different tasks in relation to children. Located this differently in different professional positions this also means that the different professionals have different access to the children, which means that their knowledge about the child will also differ. Several studies present how the opportunities and dilemmas in the collaboration relate to the professionals´ positions and opportunities for influence and access (Morin 2016; Knotec 2003; Røn Larsen 2012; Edwards 2009; Hjörne & Säljø 2014). Linked to the distributed character of professional work is the question of access, power and disposal. Influence in collaborative practice is therefore also a question of positions and resources, due to the distributed character of inter-professional collaboration. At one of the workshops that I observed, one of the participants, a social worker, made the following comment about inter-professional collaboration not being a power-free space. She said:
“It is very important who sits at the end of the table at the meeting. Who is the first speaker? I think that you also have to consider how we can get the marginalised voices into play. Many teachers say they do not actually understand what the psychiatrists are saying and that they experience being cut off in the dialogue. They have their diagnostic system. It creates a distance in itself. For example, how long can the psychiatrist talk before the teachers leave? I have also seen some social workers being sent to a network meeting with an agenda from the school that they themselves do not believe will help the child concerned. Then they call in sick. We have also experienced having children sent home from the psychiatric services with a recommendation that they should be given special educational support which we are unable to provide.”
As the social worker states the inter-professional collaboration is not at power-free space. She mentions in the quote how the inter-professional meeting is framed in structural power relations by asking “who sits at the end of the table?” and “who is the first speaker?”. She mentions that the different professions inhabit very different knowledge about the child and family which may limit the dialogue as she says the psychiatrists have their diagnostic system it creates a distance in itself when for instance teachers are cut off in the dialogue because of the certain diagnostic language used by the psychiatrists. In this way structural conditions as for instance when the psychiatrist is placed as the meeting-leader and when psychiatric diagnostic language dominates the dialogue in the inter-professional collaboration results in other voices being suppressed as the voice and perspectives of the teachers. In an interview with a teacher on the inter-professional collaboration this analysis is confirmed as the teacher states:
“This and so much else, it is so characteristic of this top down processes. So it's like we are pieces in a game where someone moves us around depending on how they think we should act and where we should stand, and I think it´s problematic.”
The teacher reflects in the above on his limited experience of possibilities for influencing the dialogue in the child psychiatric center. Further more in the above quote of the social worker she mentions the inconsistencies existing between different sectors by giving the example of children being sent home from the psychiatric system with a recommendation that they should be offered special educational support by municipalities, which do not have the resources to provide this support. One psychologist employed in the field of child psychiatry elaborates on the theme of the inconsistencies at play between sectors. She says:
“We are often in different time loops. The regions make hospitalisations shorter, the patients get so much worse before they get support, or they are hospitalised four times. And the workflow in school psychology is very slow. The psychological assessments and reports from the school psychologist can be a delaying factor in getting started. We see children who are school refusals on 2nd year because the schools have to make strict priorities. It will be late before the case proceedings begin, it would be super nice if the municipality could work concurrently. The children are lost before they are even given an offer of support.”
This quote reveals that structural divisions between regions and municipalities limit opportunities to work holistically and create coherence in professional collaboration on initiatives aimed at children in severe difficulties. The main obstacle is that the sectors involved are often described as being “in different time loops”.
The professionals who contribute to collaborative processes typically have different tasks and positions, which means that they have different access and availability (Dreier 1999; Morin 2007) in relation to the process involved in making decisions about possible interventions. The concept of access refers to an individual’s share in relation to resources and living conditions (Holzkamp 2005). The empirical quotes mentioned above reveal that the professionals involved in collaboration do not have the same knowledge about children, and that the knowledge they possess is closely linked to their location, the tasks they perform, and therefore their professional position. The view of the child in difficulty and of what efforts and interventions are considered relevant is in this way linked to the different professional’s availability, access and direction in the collaboration. This means that the professional’s perspectives, interests, tasks and knowledge of the child are mediated through their personal located participation in action contexts. Hence, the professional knowledge and view of the child, the kind of problem and possible problem solution or intervention from this perspective may vary a great deal in the collaborational practice as the professional judgement is made from a certain location and position with certain often specific and limited access to knowledge of the child. With the concept of social inequality, attention shall be drawn to the social distribution of opportunities for taking part in and influencing the inter-professional collaboration often times linked to conflicts about how the difficulties should be understood, how it should be handled and who has the responsibility (Højholt 2017). As already shown more of the informants in the development project mentions how the inter-professional collaboration is framed in structural power-relations and how inconsistencies among sectors are at play. In what follows I will unfold the focus of these inconsistencies in the above referred to as “we are often in different time loops”.
3 Lost opportunities and dilemmas – when the systems used by different sectors are not coordinated
One of the child psychiatrists participating in the development project mentions a model used for guiding the process of early interventions in municipalities which is called “the intervention ladder” as an example of how different approaches and organisational differences create inconsistencies between sectors which hinder the provision of timely help for children and families. The intervention ladder is a standardised model for reorganising practice procedures aimed at early preventive support and intervention used as a tool in the municipalities, for instance by school psychologists. The intervention ladder focuses on scaffolding how “qualified efforts can be made earlier that support children or young people’s development and connection to everyday life” (National Board of Health and Welfare[2], see Figure 1).
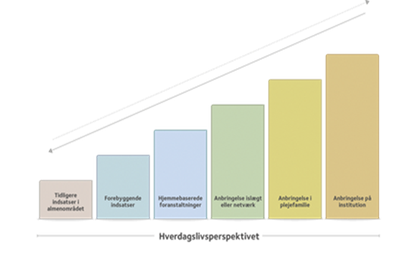
Figure 1: The intervention ladder[3]
In the model, there is a focus on ensuring that interventions match the needs of the child and family concerned, bringing the child as close to a normal everyday life as possible. In the empirical material on early inter-professional and cross-sectoral collaboration, the intervention ladder is central to discussions about support. Many of the professionals involved in the development project, particularly the school psychologists, regard the model as a working tool in their practice, which provides a framework for understanding the difficulties of children and families and seeing these in relation to organisational opportunities for support. However, as mentioned in the interview above, the child psychologist identifies a few dilemmas related to the application of the model when it comes to making decisions about the child’s best interests in the collaboration between professional disciplines and sectors. This is described in the following in connection with the collaboration on for instance the diagnosing process. The model may in certain cases promote a discrepancy in the collaboration between the sectors, which may have an impact on the possibility of timely and relevant action. The psychiatrists say that they sometimes discharge children and young people after a lengthy stay in hospital without a decision having been made regarding ways of supporting these young people when they return to the municipality in which they live. The logics relating to the intervention ladder seem to play a role here, as explained by one psychiatrist:
“Structurally, it’s all about making the smallest possible intervention. The municipalities have to try out for instance school based intervention close to the everyday environment , and if that’s not enough then you have to try something more comprehensive and massive, and if that’s not enough then you have to try something even more extensive. And with the greatest respect, we do sometimes have some young people where we can see that it may well be they have received support but it is not enough. It will worsen their situation to have to go through all these steps in the ldder, and I wish we could say: then we go in with psychiatric intervention now for half a year or a year or how long it takes and then we can go down again to lesser precautions. Because right now it's just another burden to try what does not work and what does not work and what does not work and maybe then you end up with a young person who is not receptive to what could have worked. So it’s the logics in the model which get in the way and you end up having to go through all the steps chronologically, leading to a worsening of the child’s condition. In our system, we really know something about the young people when they have been hospitalised for eight weeks where I can have a feeling that the municipalities will run their own course and process themselves. They will get to know the young person themselves and they will draw their own conclusions, but this will have consequences for the young person. It often results in two parallel courses. In terms of time, it becomes very extensive where we may need some action here and now. We describe, for example, a need for 24-hour treatment and support and then the municipality chooses to organize a preventive support only in the school which makes the young person worse off over an entire year. They start from the bottom of the ladder.”
As pointed out in this interview, the logics in the intervention with a focus on the smallest means letting the child remain as close to everyday school life as possible sometimes mean that interventions come too late and that the young person concerned may get worse during that period. So what is being described here is that the model itself may lead to long courses with the child/young person growing worse before support is provided. The description of the way in which the intervention ladder is implemented in the municipalities seems to address also questions of negotiation of problem understandings and who has the power to define as well as what is the problem and how shall it be treated. The child psychiatrist continues:
“A young person comes in and we may sow a seed but then we meet a municipality that says: Well, they just need to feel a bit better first. This is frustrating because you know that this young person will go back home and sit in front of the computer once again without getting any help for six months. Then they are lost. It doesn’t make sense for such young people. The seed that we sow will only grow if children get the right services, even if it is expensive”.
When the psychiatrist says: “I can have a feeling that the municipalities will run their own course and process themselves” or “They just need to feel a bit better first”, this is an indication that even though there has been an eight-week hospitalisation in psychiatric care, followed by different kinds of knowledge sharing across the region and municipality, it is indicated that differing exploration trajectories and problem understandings might be at stake. When it comes to establishing an intervention offer for the young person which is the responsibility of the municipality the intervention ladder and the logics related to this model, often leads to a new process of exploration of the young person’s situation and to establishing support of a quite different character than what the course in the child psychiatric center indicates. Different understandings and logics in the sectors in this way influences and might hinder timely and as the psychiatrist indicates relevant help. The result is a lack of coordination across sectors which increases the risk that resources will be wasted, as also described by Shahidullah (2019). The problem is that a structurally adopted model, in this case the intervention ladder, will set the structural framework for how the investigation procedure is approached in relation to children and young people. As it is elaborated: There will be two pathways in the system which is time consuming where there may need action here and now to prevent a worsening of the problem. As the above have shown structural differences relating to different knowledge positions of how to approach intervention strategies across sectors results in dilemmas and risk of lost opportunities to support children, young people and families by timely action and relevant intervention.
4 Conclusion
The intention of this article has been to analyse the ways in which institutional and organisational dilemmas and inconsistencies across welfare sectors might lead to suppressed voices and lost opportunities in early inter-professional and cross-sectoral interventions. The analysis shows that when sectors are arranged on the basis of different systems and organisational procedures, dilemmas may arise when it comes to providing timely and relevant support for children, young people and families. Different understandings and logics in the different sectors influence inter-professional collaboration, the result being a lack of coordination across sectors leading to an increased risk that resources will be wasted. Focusing on organisational challenges in inter-professional everyday professional practice, the analysis has discussed difficulties in providing timely help and resources for children and families who are in contact with the psychiatric system. The analysis showed how the inter-professional collaboration is framed in structural power-relations as for instance when the psychiatrist is placed as the meeting-leader and when psychiatric diagnostic language dominates the dialogue in the inter-professional collaboration resulting in other voices being suppressed as the voice and perspectives of the teachers. The analysis also showed how inconsistencies among sectors are at play as different professions inhabit very different knowledge about the child and family. This may limit the dialogue as seen in the analysis where the language of the diagnostic system creates a distance in itself when for instance teachers are cut off in the dialogue because of the certain diagnostic language used. In this way, the empirical analysis shows that situated inequality in professional practice as part of structural conditions and dilemmas may result in suppressed voices and lost opportunities in early inter-professional and cross-sectoral interventions.
As the analysis has shown, structural differences across sectors result in dilemmas and the risk of lost opportunities to support children, young people and families by timely action and relevant interventions, as pointed out referring to the intervention ladder model and different tasks that set the guideline for exploration and intervention procedures across sectors. The analysis shows that these dilemmas are linked to the way in which the different professionals and systems work together. Causing very long time courses for the treatment and intervention but also different views of what is the problem and how it shall be solved. In more general terms the analysis of the inter-professional collaboration between sectors draws our attention to the fact that inter-professional collaboration by virtue of its character is a forum in an often time-consuming process with parallel processes. The collaboration is largely connected to and depending on what has taken place in other contexts where the various parties have been involved in a collaboration with child / family and each other as part of clarification and / or investigation process. The inter-professional and cross-sectoral collaboration therefore requires far more than that what lies in a traditional expert understanding, where the parties primarily work with their own professionalism and individual tasks. With a look at the inter-professional meeting as part of a time-consuming process that involves the contribution of different disciplines in a plurality of contexts, but also precisely a meeting across these contexts, an important part of the attention is related to the inter-professional collaboration on children in difficulty therefore is to conceive of what here shall be addressed as the social arrangement of collaboration. A social arrangement can be defined as the scheme of a context and the connections between contexts for the procedure of certain practices such as collaboration on children in difficulties (Dreier 2011). Ie. that certain rules, frameworks and procedures influence and shape the direction and dynamics of individuals' participation and in the collaboration on a specific pedagogical goal. The arrangement of a context often defines which persons are considered to be legitimate participants. In addition, the arrangement often involves certain social positions for the participants due to special personal backgrounds such as ownership, employment, competencies, membership and kinship. People's activities and the relationship between people are part of the social context that takes place in special social contexts and is influenced by their social events. Social events are both connected but also separated in ways that are both reproduced and changed over time in a dynamic between the participants including the participants' access and framework, rules, procedures, goals and means. Contemplating the social event of the collaboration will therefore mean that the participants in the collaboration relate to the inter-professional and cross-sectoral meeting as part of a process across sometimes many different work-flows, objectives and interests placed in contexts other than the professional context in which the professional is participating. Therefore, this also requires an awareness that the inter-professional meeting is a meeting where both own and other professions' agendas and tasks are at play. In this regard, Edwards emphasises that in inter-professional collaboration it is important that different professionals have access to each other’s different motives, values and positions also as part of political agendas and logics, because otherwise negotiations and discussions about a child’s potential, development and learning opportunities “… are likely to become formulaic rather than responsive and fluid” (Edwards 2009, p. 38). Edwards emphasises the importance of focusing and working in ways which ensure that the resources of other disciplines can be part of the process, and calls this a decentralisation of individual expertise (Edwards 2009). With these perspectives in mind, part of the professional expertise and role in an interdisciplinary collaboration will be to be able to transcend one's own professionalism and own perspectives. Against this background, it is worth pointing out that the priority in the collaboration is to free up resources so that one or more professionals can play a coordinating and facilitating role, which includes outreach work to transcend contexts with a view to bringing different parties, professions and sectors together to cooperate in relation to specific children and families. The development project in which the empirical findings of this article are anchored is a response to some of the dilemmas analysed in this article. As part of the development project, new workflows are being tested where collaboration between sectors is sought to be made more flexible and a new standard tool has been developed for the use of enhancing the information flow across sectors. This developmental work gives some reason to hope that some of the dilemmas analysed in inter-professional collaboration between sectors could be dealt with, and that new opportunities for timely and relevant support could be created.
References:
Cole, M. & Engeström, Y. (1993). Distributed cognition – A cultural Historical Approach in (eds. Gavriel Salomon) Distributed Cognitions – Psychological and Educational Considerations (pp.1-46). Cambridge University Press, Cambridge.
Dreier O. (2011). Personality and the conduct of everyday life. In Nordic Psychology, 63 (2). 4-23.
Edwards, A. (2009). Relational agency in collaborations for the well-being of children and young people. I Journal of Children’s services. 4 (1). 33-43.
Engeström, Y. (2018). Expertice in Transition. Expansive learning in medical work. Cambridge University Press.
Hamre, B., Hedegaard-Sørensen, L. & Langager, S. (2018). Between Psychopathology and Inclusion: the challenging collaboration between educational psychologists and child psychiatrist. International Journal of Inclusive Education. 22 (6), 655-679.
Hartnell, N. (2010). Multi-disciplinary Approaches to Pupil Behaviour in School – the Role of Evaluation in Service Delivery. Educational Psychology in Practice. 26 (2).
Hjörne, E. & Säljö, R. (2014). Analysing and preventing school failure: Exploring the role of multi-professionality in pupil health team meetings. International Journal of Educational Research. 63, 5-14.
Holstein, B. Henriksen, T., Rayce, S., Ringsmose, C., Skovgaard, A.M., Teilman, G. K. & Væver M. S. (2021). Mental sundhed og psykisk sygdom hos 0-9 årige børn. (Mental health in 0-9 year old children) Vidensråd for forebyggelse.
Holzkamp, K. (2005) Mennesket som subjekt for videnskabelig metodik. (The person as subject for scientific methods) Nordiske Udkast. 33(2) 5-33.
Højholt, C. (2005). Forældresamarbejde – Forskning i fællesskab, (Parent collaboration – joint research) Dansk Psykologisk Forlag, Gylling.
Højholt, C. 2011 (ed.). På tværs af familiearbejde og inklusion i skolen. (Across family work and inclusion in school). Dansk Psykologisk Forlag.
Højholt, C. (2016). Child, families and communities. The Netherlands: Springer Netherlands.
Højholt, C. (2017). Situated Inequality and the Conflictuality of Children´s Everyday Life. In Psychology and the Conduct of Everyday Life (2017). Ed. Højholt & Schraube. Routledge. New York.
Knotek, S. (2003). Bias in problem solving and the social process of student study teams: A qualitative investigation. The Journal of Special Education, 37, 2-14.
Krops, N. P. & Marlone, D. (2004). Interdisciplinary practice in developmental disability. Journal of Social work in Disability and Rehabilitation. 3(1). 21-36.
Law, C. E. & Woods, K. (2018). The representation of the management of behavioural difficulties in EP practice. Educational Psychology in Practice. 34 (4). 352-369.
Lave, J. (1985). The Social Organization of Knowledge and Practice: A Symposium. Antropology and Education Quarterly. 16(3): 171-176.
Lave, J. & Wenger, E. (2005): Practice, Person Social World. In (Daniels, H., eds.): An introduction to Vygotsky. New York: Routledge.
Røn Larsen, M. (2012). A paradox of Inclusion: Administrative procedures and children´s perspectives on difficulties in school. (Hedegaard, M.; Højholt, C.; Skjær Ulvik, O.; Aronsson, K., ed.) Children, Childhood and Everyday Life: Children’s perspectives: Information Age Publishing, incorporated.
Maki, E. D., Sheppard, A., James, J., Mueller, M, Broadhead, S., Brodsky, L., Couse, A., Pearrow, M. (2019). School Psychologists perceptions’ of systems Change: A Case Study. School Psychology Forum. 13 (1). 41-52.
Moola, N. & Lazarus, S. (2014). School psychologists’ view on challenges facilitating school development through intersectoral collaboration. South African Journal of Education. 34 (4).1-10.
Morin, A. (2011). Samarbejde om inklusion. På tværs af familiearbejde og inklusion i skolen. (Collaboration on inclusion. Across family work and inclusion in school). C. Højholt (ed.). Dansk Psykologisk Forlag.
Morin, A. (2016): Et positioneret samarbejde: på tværs af skole, PPR og psykiatri. (A positioned collaboration: across school, school psychology and psychiatry). Inklusion, udsathed og tværprofessionelt samarbejde. B. Hamre; V. Larsen (ed.). Frydenlund Academic. 107-124.
Morin, A. & Hedegaard-Sørensen, L. (2018). Psychiatric testing and everyday school life: collaborative work with diagnosed children. Testing and Inclusive Schooling – International Challenges and Opportunities (Ed. Hamre, B., Morin, A. & Ydesen, C.). Routledge.
Mørck, L.L, and Hunniche, L. (2006). Critical psychology in a Danish context. Annual Journal of Critical Psychology, 5.
Ofstedal, K. & Dahlberg, K. (2009). Collaboration in student teaching: introducing the collaboration self-assesment tool. Early Childhood Teacher Education. 30(1). 37-48.
Shahidullah J.D. (2019). Behavioral Health Care Coordination Across Child-Serving systems. A Burgeoning Role For School Psychologists. In School Community Journal, 28, 1. (279-296).
Szulevicz, T. (2018). Psychologists in (Neoliberal) Schools - What kind of Marriage? Integrative Psychological and Behavioral Science, 53(3). 329-339.
The Danish Government https://www.regeringen.dk/media/4291/aftale-satspuljen-sundhedsomraadet-2018-2021.pdf.
Indsatstrappen (the intervention ladder) https://socialstyrelsen.dk/tvaergaende-omrader/socialstyrelsens-viden/redskaber-til-styring-og-udvikling/indsatstrappen-1.
Social- og Indenrigsministeriets Benchmarkingenhed (2020). Udviklingstendenser i forhold til børn og unge med psykiatriske diagnoser. (The Benchmarking Unit of the Ministry of social and domestic affairs. Developmental tendencies related to children and young people with diagnoses).
The Municipalities/Kommunernes Landsforening (KL). Udsatte børn - nøgletal 2019 (Vulnerable Children – key figures). https://www.kl.dk/media/18776/noegletal-de-udsatte-boern-og-unge-2019.pdf.
Whyte, W. F. (1991). Participatory Action Research Through Practice to Science in Social research. Participatory Action Research, Sage, London, 1991.
Author´s
Address:
Anne Morin
Aarhus University
Tuborgvej 164, 2400 København Nv.
+4525130708
amt@edu.au.dk