Achieving good outcomes in foster care: a personal perspective on research across contexts and cultures.
June Thoburn, University of East Anglia
1 Introduction
The context of this ‘personal perspective’ is the 20 plus years of collaborative research on children in care undertaken with colleagues from Australia, England, Israel, Italy, Norway and the USA but also drawing on learning from colleagues from the 28 jurisdictions who assisted with my data-based study of children in care in 28 jurisdictions (Thoburn, 2010a; Thoburn, 2010b; Thoburn, 2013). My perspective was enriched and up-dated by the papers presented at the 2015 Siegen foster care research conference, some of which are included in this volume. It remains, however, a personal perspective from an English social work practitioner, educator and researcher, who is more familiar with the UK conducted research and publications in the English language. Given the breadth of the foster care research now available, the choice of areas to be covered is also a personal one. In an attempt to cover the foster care research ground, first in the short concluding paper to the conference and now in this paper, I have done rough justice to the extensive research findings now available. The overview is also partial in that it draws on data from high income rather than middle or low income countries, but the analytical framework is close to that used by the UNICEF Better Care Network framework recommended for high and low income nations alike. (Better Care Network, 2009). There are of course still many gaps, which are pointed to in the discussion sections and conclusion.
2 The service planning and research processes
The paper uses a ‘logic model’ for understanding both the service provision processes and the research methodologies (Figure 1). It moves backwards from a consideration of the outputs and outcome measures used by service planners and researchers, to an exploration of how these may differ depending on the aims of the foster care service in different countries. The foster care knowledge base on the processes of fostering and on supporting foster families (what does research tell us about ‘what is in the black box’ of day to day practice) is then considered in the light of any differences in aims and child characteristics.
Outputs and Outcomes
Rich and poor countries alike share a commitment to meeting the needs of all children as set out in UN Convention on the Rights of the Child (United Nations, 1989) and the many subsequent documents. Birth and/or alternative parents and carers must meet the basic human needs as summarised by Maslow (1954) for:
· Adequate nutrition and shelter
· Protection from danger, including all types of abuse and neglect
· Health care
· Opportunities and encouragement to learn.
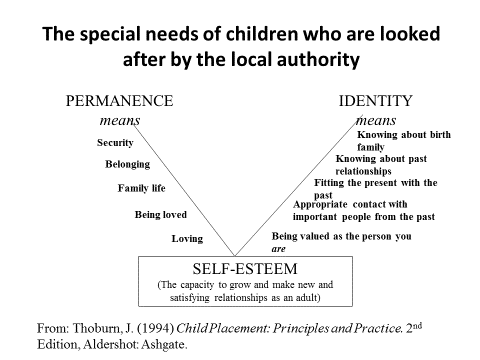
Those in rich countries had come to think of failure to meet these basic needs as in our past. Regrettably, in several high income and transition economies, public service cuts encouraged by neo-liberal philosophies and austerity policies (in England specifically targeted on those reliant on social security benefits) are making it more difficult for families to meet their children’s basic needs. If placement in care becomes necessary, returning children to their birth families is becoming more difficult because of the growing gap between the standard of care to which they become accustomed in foster care and the poverty and poor environments many will return to. Material neglect resulting from absolute poverty and inadequate housing (visible in the shape of unheated homes, shoes that don’t fit and reliance on food banks) is increasingly likely to be part of the lived experience of children who return home, contributing to further instability if they have to return to care. (Farmer et al, 2011; Wade et al. 2011, Thoburn et al. 2012; Featherstone et al, 2013). But for children who need more than a short stay in care, all countries recognise the additional needs (summarised in Figure 2) for a ‘sense of permanence’ and a ‘sense of identity’ (Thoburn, 1994).
So to summarise, though there are differences in emphasis and prioritisation depending on country, context and research design, the wellbeing outcomes that policy-makers seek to achieve, and researchers seek to evaluate are:
· Physical, emotional, ‘educational’ wellbeing into adulthood
· Stability- keep any moves to a minimum
· A sense of permanence
· Family membership (foster family and birth family)
· Continuity – links with relatives, friends and community
· Minimum length of stay in out-of-home care (a key aim in USA and UK policy but less apparent in other countries (Skivenes and Thoburn, 2016)
· Normality – but different family forms including being part of a foster family should not be seen as conveying the stigma associated with the ‘abnormal’, as recounted by several of the presenters at the Siegan workshop who reported on children’s views.
The papers in this volume and delivered at the Siegen seminar, illustrative as they are of the knowledge base on foster care across national boundaries, demonstrate similarities and differences in the way policy makers and researchers in different countries make different decisions about outcomes to be prioritised, measured and reported on. These differences are related to differences in historical and cultural context, and political as well as professional choices (Gilbert et al. 2011; Thoburn, 2013). As an example, different choices are made about whose outcome is to be measured. Figure 3. All policy makers and researchers maintain that it is the outcome of the child/ren in need of foster care placement that is to be measured- all have in their legislation, in line with the UNCRC, that the child’s welfare must be a paramount consideration, and that children’s views should be heard and taken seriously. And most social service agencies recognise a ‘duty of care’ and a ‘right to a fair hearing’ of the adults to whom they provide a service or who are likely to be impacted on by the service provided to a child. But the attention paid to the wellbeing outcomes for birth mothers and fathers, siblings, foster carers and adopters both in the services provided and the research undertaken differs.
Some of these ‘outputs’ listed above are not child wellbeing ‘outcomes’ but can be useful proxy interim outcomes if longer term outcome data is not yet available. Multiple changes of placement (placement instability) comes through in qualitative studies as a proxy for a poor outcome, at least in terms of what young people have to say about their experience. But young people contributing to research report that one or even two moves as teenagers from placements that were not working for them could be followed by more successful placements (Schofield, 2003). Sadly, it appears to be getting harder to persuade funders to fund longitudinal studies, although some researchers have been able to ‘pick up’ cohorts at regular intervals (Moffatt and Thoburn, 2001; Bullock et al , 2006; Schofield and Beek, 2009)
Where it is possible for researchers to follow foster children into adult life ‘self esteem’ as an adult and the ability to make satisfying relationships in adult life are generally accepted as indicators of a successful outcome. Because most children entering care will have additional obstacles and challenges to overcome, it is generally agreed that wellbeing outcomes cannot be assessed until young people are well into their 20s. Take educational achievement, for example, a young person entering care at 15 in part because of school problems is unlikely to by having good exam results 18 months later, though he or she may well pick up their education at 18 and go through college and gain qualifications in their twenties.
Some measures listed above are ‘outputs’ and some have more relevance to political or economic goals than child welfare outcomes. In the UK and USA, being in care is, in the eyes of many politicians and the public, a ‘last resort’ because it ‘causes’ poor outcomes. The sub-text of much discourse on children in care is ‘keep them out of care if you can, and if you can’t, get them out as quickly as possible’ (Cameron, 2015). This prevailing view is not supported by research going back over the years (the latest being Sebba et al, 2015)) and earlier summarised by Bullock et al (2006), Biehal et al, 2010; Thoburn and Courtney (2011) and Boddy (2013). Whilst qualitative studies provide evidence that the care system badly fails a minority of those who enter care, the majority (both in the eyes of the young people themselves (Office of the Children’s Commissioner, 2015) as well as research reports using quantitative and standardised measures, do as well or better than if they had remained at home or returned quickly home. Those who go home too quickly, have inadequate support, and return to care on more than one occasion do least well. This is an example of an ‘output’ not shared across all countries. Most European countries have tended to view placement in care as a positive response in appropriate circumstances, although more governments seeking to cut public expenditure are calling into question why so many children need to be in care. This is one reason why the use of the most expensive placement (residential care) is declining across Europe and foster carers are caring for children and young people with very complex needs who would previously have been placed in a residential setting
2.1 Who needs a foster care service in different countries?
With respect to the foster care service (as distinct from the characteristics of foster families) the main differences in the ways in which policy makers in different countries seek to achieve good outcomes for children who need a foster care placement are:
· the extent of use of foster care compared with other placement options such as residential care
· the proportion of children entering care via the courts, administrative procedures or through agreement with parents
· the ages of children entering care, which is linked to the availability of family support provision for the different age groups.
Taking the last of these first, table 1[i] shows that in the Anglophone countries (illustrated here by data from the USA and England), a much larger proportion of care entrants is under 4, and this is especially the case for the under 12 months age group. Though all countries must appropriately provide for children in each age group, the table illustrates that the care services in Germany and Denmark and other similar countries have to be ready to care appropriately for smaller numbers of infants and larger numbers of teenagers than is the case for the USA and English service agencies. So, looking at figure 1, the entrants to the care system differ with respect to age group, and with this comes other differences in the needs that the care system has to meet. One explanation for these age group differences is that some countries (the Nordic countries are a good example), have a combination of more robust universal services such as day care, and in some cases lower thresholds for the receipt of ‘targeted’ social work and other services in the home. It can be hypothesised that when pre-school or school age children do come into care, much more has been tried so that it is less possible to get children safely home than in countries with less well developed family support services and higher thresholds for receipt of in home targeted services (Skivenes &Thoburn, 2016)) . On the other hand, being older at entry to care and having had more time to put down roots in their extended birth families and communities, despite problems of parenting or family relationships that resulted in the need for care, the children themselves may be less willing to have all their links severed.
Table 1 Percentages of those entering care by age group* **
|
Country |
0-4 (<12 months) |
5-9 |
10+ |
|
England |
35% (17%) |
18% |
47% |
|
Denmark |
12% (5%) |
12% |
76% |
|
Germany |
15% (0-5 yrs) (4%) |
28% (6-11 yrs) |
56% (aged 12+) |
|
Sweden |
12% (0-3 yrs) |
15% (4-9 yrs) |
79% |
|
USA |
38% (15%) |
20% |
43% |
*years for these data range from 2010-2013 **Data on entrants to care during a given year are not available from some countries, although data on children in care on a given date are usually available. It is data on entrants which more clearly indicate how the foster care service is being used.
Table 2 % of children in care in different placement types
|
|
England |
Norway |
Denmark |
Sweden |
USA |
|
Non-kin foster care |
63% |
55% |
60% |
65% |
46% |
|
Kinship foster care |
11% |
17% |
Included in above |
12% |
23% |
|
Adoption |
5% |
|
|
|
5% |
|
Residential care |
12% |
14% |
39% |
21% |
19% |
|
Other |
9% |
14% |
1% |
3% |
4% |
Table 2 shows that, unsurprisingly, there is a greater use of residential care and a consequently lower use of foster care in those countries where a larger proportion of care entrants are already teenagers. A consequence of this difference is that, although proportions and absolute numbers of pre-school children entering care are lower in most European countries than in North America, UK nations and Australasia, these younger entrants are more likely to stay for longer periods in their foster families. If we look at a population of children in care on a given date, more will have joined their foster families at a young age and be still there after several years than is the case in the UK and USA where young entrants to care are likely to leave quickly via adoption or guardianship. When adoptions from care do happen in Europe, this is most likely to be by their existing foster carers with whom they have lived for some time.
Differences between countries with respect to the legal and administrative processes that result in placement are less easily explained and may be more a factor of ‘custom and practice’ (see especially the edited book by Fernandez and Barth, 2010). Norway, Sweden and Denmark have much in common but in Sweden and Denmark more children come into care as a result of social work discretion and with parental agreement than is the case in Norway.
3 The foster care services
Moving onto the detail of the foster care services (the ‘what is in the black box?’ part of the logit model) it is not surprising given these age and other differences, that Denmark and Germany place more children in residential care settings and consequently fewer in foster family care. If we look at Figure 2 and the aim of providing a ‘sense of permanence’ it is also unsurprising that countries with a larger number of older school age entrants to care tend to use terms such as stability and continuity of relationships, whilst England and the USA with their larger number of infant care entrants (and with most prospective adopters wanting to adopt infants or toddlers), place more children from care for adoption, and are more willing to do so by over-ruling parental wishes. These two countries tend to emphasise ‘legal permanence’ and exit from care via adoption or legal guardianship. However recently in England a set of meetings between senior civil servants and foster care researchers, has resulted in new statutory guidance on care planning which dropped the term ‘legal’ from the official definition of ‘permanence’. This change was informed by the evidence from data analysis and longitudinal studies (Sinclair et al, 2007; Biehal et al, 2010, Biehal, 2014) that adoption is a ‘permanence’ route for only a small minority of care entrants, and research studies that concluded that, provided that placements are made initially or confirmed as ‘permanent’, long term foster care can have positive long term outcomes (Schofield and Beek, 2009; Biehal et al, 2010).
In 1989 Jane Rowe, a researcher on foster care who had a major impact on those of us who followed her, drew from a large scale mixed methods research study the following list of foster care roles and tasks, which has subsequently been used with respect to more recent studies of foster care (Sinclair et al, 2006; Thoburn, 2010 Bullock this volume)
· Emergency care
· Planned temporary care / strengthening families/ preparation for reunification
· Regular series of placements with the same family (‘respite’ or ‘support’ foster care, often for disabled children)
· Assessment (of child, of parents, of whole family)
· Therapy (of child, of parents, of whole family)
· Preparation for long-term placement, usually of young children and usually with an adoptive family not previously known to the child
· Care and upbringing (‘long-term’ ‘permanent’ foster family care)
· A bridge to independence for teenagers entering care following family breakdown or following an adoptive or long term foster family breakdown.
At the extremes, one foster care career might involve the upbringing of a single foster child or sibling group as ‘part of the family’ for 16 plus years and on into adult life; another foster care career might involve 30 or more children staying for different lengths of time, some becoming long term members of the family, others being helped to go safely home; and another might involve 30 or more infants and children arriving in an emergency and moving on to an adoptive or long-term foster family.
Some countries differentiate more than others between service needs for different ‘foster care careers’. Although it is clear from the studies represented in this volume that there are many similarities in the way in which foster care services recruit, assess, train, match children with foster carers, and support foster families, some countries differentiate more than others in the way they adapt the service to the intended role of the foster carers. The foster care career where there is most similarity across boundaries is therapeutic foster care for older children with challenging behaviour. This was first introduced in Sweden as ‘professional foster care’ in the 1980s and most recently provided as a manualised programme- Multidimensional Treatment Foster Care (MTFC) (see Chamberlain, 2003 and the evaluations in England and Sweden by Biehal et al, 2011 and Hansson and Olsson, 2012).). In some countries, researchers report an uneasy tension between the supposed aim of reunification and the reality that the foster carers have become foster parents, and the child wishes to be assured that he or she will remain part of the foster family. The emphasis on children’s need for a sense of permanence in England has resulted a recognition of the differences between ‘task’ focused’ foster carers and ’family for life’ foster parents. There is, however less emphasis on ‘shared parenting’ ‘therapy’ and foster care as family support, than in most European countries. As noted earlier, Farmer et al, (2011), Wade et al. (2011), and Thoburn et al. (2012) have called attention to the poor outcomes for children returning home from care and recommended that task centred foster carers should have a bigger role in working with birth parents when the plan is for children to return home Although in theory, one might anticipate that countries which emphasise the importance of birth family links might recruit, train and support foster carers who can empathise with and have particular skills in working with birth families, it is not at all clear from the body of research that this happens (an exception is reported in Fernandez, 2012; Fernandez and Lee, 2011, )
4 The foster families
4.1 Foster care careers
The knowledge base on motivations, values, qualities skills and support needs of successful foster carers/ foster parents has increased greatly in recent years with evidence in the papers in this volume of researchers in different countries working together or building on each other’s work. This paper cannot attempt to summarise this now extensive volume of work but draws on my above observations about foster care service aims to draw out some reflexions.
Some of the skills needed by successful foster carers are shared across all the different roles and foster care careers. For example, the ability to empathise with the child and also with the birth family is as essential for long term foster carers who go on to adopt (even those who have little or no contact with birth parents) as it is for treatment foster carers. Enjoying being with children and also being able to rise to (and even enjoying) a challenge is an attribute that all those caring for children placed from care are likely to need to draw on at some point. Neil et al (2014) found that even amongst children mostly under 2 when placed for adoption, only around half were ‘thriving’ between 16 and 18 years after placement and that many were demonstrating seriously challenging behaviour.
On the other hand, some attributes are more important to some foster care roles than others. The ability to be part of the therapeutic team, and to value this part of their role, is essential for treatment foster carers. ‘Family for life’ foster carers need to be able to work with professionals, but there are examples in the qualitative research literature of foster parents standing up for and advocating for their child, whose disagreements with the professionals led to negative annual appraisals and even removal of the children sometimes against the wishes of the child. Sometimes a change of social worker, at the request of child or foster parents, has led to a positive resolution of the point of disagreement. Schofield and colleagues (2013) explore this question of different role identities in their longitudinal studies of long term foster carers.
They conclude that successful long term foster parents can have different role identities, but there must be an element of each. Some identify primarily as foster carers, but also embrace the role of parent; others primarily identity as parents, but also embrace the professional elements of their role of foster carer.
Countries which recognise the differences between different foster care careers tend to be more relaxed about the discourse of the service – is ‘foster carer’ the required term to be used by social workers and in official reports, and ‘foster parent’ frowned on? Does the increasing recognition of the importance of children’s rights recognise that some will want to call their foster parents ‘mum and dad’ – though they usually also want to continue to refer to their birth parents as ‘mum and dad’.
Other important recent contributions to the knowledge base on the characteristics of more and less successful foster carers (including studies of foster home breakdown) look at ways of improving the involvement of children, foster carers and birth parents in both long-term decision-making (in the England guidance referred to as the ‘permanence plan’ and the aspects of daily life (the ‘placement plan’). The use of names just referred to is an example and in the course of the conference we heard examples from qualitative studies of young people who in some circumstance wanted their foster parents to introduce them as ’my foster son’ but mostly as ‘my son’.
5 Outputs, outcomes and the research agenda
The breadth and complexity of the foster care knowledge base bears witness to the complexity of the service, provided as it mostly is over long periods with many different ‘interventions’ and individuals with the potential to impact on outcomes. The variables associated with good or poor outcomes that have been identified and studied by different researchers concern:
· the child,
· the child’s family and biography
· the professional status, and characteristics of those providing services to the children, their parents and carers
· the approaches and methods used by social work and other services
a. decision making
b. placement practice/therapy
· law, systems and procedures for care planning, review and service delivery.
There are papers in this volume that touch on each of these, and helpful overviews are to be found in the edited volumes of Schofield and Simmonds (2009) (mainly UK) and Fernandez and Barth (2010) (covering several countries).
One aspect, sometimes touched on by researchers, but not often a major focus (but see Dance et al, 2010 with respect to adoption) is ‘matching’. My own view is that this deserves more attention than it gets, and especially has to be related to the role the foster carers are expected to perform in the child’s life. More attention is paid in the literature to the ‘skills’ of foster carers, and clearly parenting skills are important. But these can be learned, whereas motivations of the potential carers and the special needs of the child are more fixed - though they sometime change over time. Drawing on my own qualitative studies of long term foster care and adoption and those of others, I conclude that matching the needs and wishes of the child with the motivations/aspirations of the proposed carers (and taking into consideration the hopes of birth relatives about the role they can continue to play in their child’s life) is essential to successful long term placements, but often gets left out of a check list of necessary skills and attributes.
Given the complexity of the foster care service and the diversity (in every sense of the word) of foster families, it is unsurprising and appropriate that, as evidenced in this volume, the full range of research methodologies is used. It is to be welcomed that (on the evidence of papers presented at the Siegen workshop) we have moved on from a hierarchy of research methodologies (with systematic reviews and randomised control trials as the gold standards), both for scoping the relevant literature and for the research process itself. Practitioner and action research, the involvement of peer researchers, the satisfaction of children or adults as outcome measures (all in evidence in this volume or at the workshop), do not fit easily into ‘pure model’ methodologies. The resulting reports do not always appear in web-based searches and may require some detective work and lead-following before they come to light. There is a space for soundly conducted randomised control trials when there is a clearly identified group of children with similar needs and a specific intervention, with outputs and outcomes that can be robustly identified and measured within a reasonably short time frame. Advances in statistical techniques have also been important for the more rigorous analysis of routinely collected administrative data as with the Sebba et al (2015) study comparing educational outcomes for children in care with similar children not in care. When these results are combined with robustly conducted prospective longitudinal studies (using mixed quantitative and some increasingly imaginative qualitative methodologies) the combined analysis can be particularly valuable. But for some of the questions for which we need answers a range of qualitative methodologies, and some exciting new techniques to engage children, carers and birth parents (texting, use of cameras) are being developed to capture the experience of foster family life.
6 Conclusions
This volume and the other studies presented at the Siegen conference give evidence of sound longitudinal, and quasi-experimental methods and qualitative studies from several countries but there are still many gaps in our knowledge about child wellbeing outcomes. Some questions posed are:
· Which comparators are to be used:
a. Children in care in other placement types? the ‘average’ child? children with difficulties but not in care?
· Which outputs can be used as proxy measures for long term wellbeing outcomes?
a. Stable placement achieved / placement breakdown?
b. Child, carers, birth family having a ‘sense of permanence’? How to measure?
c. Educational success / employment/ health/ housing?
d. Satisfaction (whose?)
e. being a part of the family’ into adult life (which family/ies)?
It has been argued in this paper that researchers have much to pass on to politicians, foster care managers, practitioners, children, birth families and foster carers about how foster care outcomes can be improved. We all have much to learn from researchers in other countries that could be usefully adapted to our own foster care services. But before reaching conclusions that what seems to work in one country will work in your own, it is essential to seek information on historical, policy and cultural contexts. What, for example is the societal opinion of foster care? Are children growing up in foster care stigmatised? (Whether ‘being in care’ is seen as stigmatising depends on foster care systems and practice as well as societal attitudes and the circumstances of the young people themselves.) Does ‘public opinion’ see foster families as ‘normal’ families putting in something extra to meet the needs of special children, or just ‘doing it for the money’? Contexts and policies also have an impact on costs and outcomes, If the care system is mainly providing for teenagers with challenging behaviour, the cost per child is likely to be higher and the proportion of ‘good’ outcomes is likely to be lower than in some countries (mainly in Eastern or Southern Europe), in which fairly young children come into care largely because of absolute poverty, family tragedy, are placed in a stable kin or non-kin foster family (or even small family group home) and remain there until they are ready to make the transition to adulthood. In England and the USA, where almost all the youngest entrants leave care quickly through return to a birth family member or adoption, those who ‘age out’ of care at 16 or 18 are likely to be the ‘unadoptable’ ones with more complex histories who are more likely to have less good outcomes.
In a sentence, child
welfare systems serving children and families with different characteristics
will have different ‘success’ rates. So to end on a message for researchers to
pass on to policy makers and service planners. There is no ‘right’ or ‘wrong’
rate of children in care. Children should not be in care if their wellbeing can
be secured, with appropriate help, by remaining with their families. But those
children who need and can benefit from care should come into care. And when
making that decision, (an important message from research and from care
leavers’ groups), we all share the duty to take seriously what children tell us
and not to over-rule their wishes unless absolutely necessary in order to
secure their safety – to do so seriously impacts on their self-esteem,
self-efficacy and resilience.
Figure 1
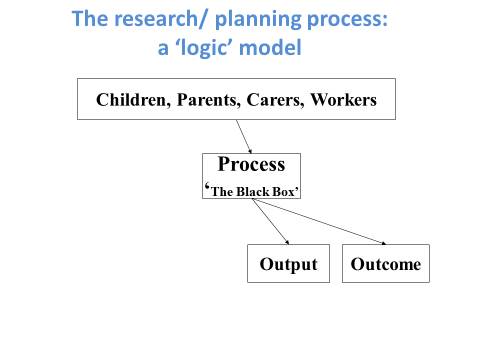
Figure 2
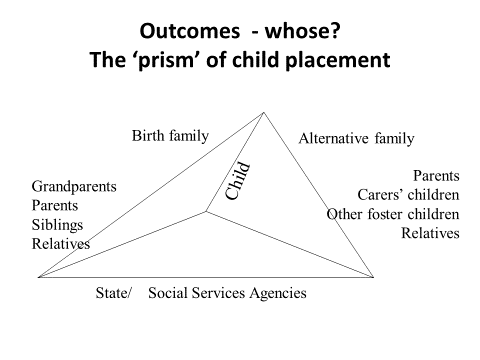
Figure 3
References
Better Care Network (2009) Manual for the Measurement of Indicators for Children in Formal Care. New York: UNICEF.
Biehal, N (2014) ‘A sense of belonging: meanings of family and home in long-term foster care’ British Journal of Social Work, 44, 4, 955-971
Biehal, N., Ellison, S., Baker, C. and Sinclair, I. (2010). Belonging and Permanence. Outcomes in Long-term Foster Care and Adoption. London: BAAF
Biehal, N., Ellison, S. and Sinclair, I. (2011). 'Intensive fostering: an independent evaluation of MTFC in an English setting', Children and Youth Services Review, 33, pp.2043-2049.
Boddy, J (2013) Understanding permanence for looked after children: A review of research for the Care Inquiry. London: The Fostering Network https://www.fostering.net/sites/www.fostering.net/files/resources/england/ understanding-permanence-for-lac-janet-boddy.pdf accessed 1.11.15
Bullock, R., Courtney, M., Parker, R., Sinclair, I. and Thoburn, J. (2006) ‘Can the corporate state parent?’ Children and Youth Services Review (Reprinted in Adoption an Fostering 2006, Vol 30 pp 6-19)
Cameron, D. (2015). We will not stand by- failing children’s services will be taken over. London: The Cabinet Office. Retrieved from: https://www.gov.uk/government/news/pm-we-will-not-stand-by-failing-childrens-services-will-be-taken-over
Chamberlain, P. (2003) The Oregon multidimensional treatment foster care model: Features. Outcomes and progress in dissemination. Cognitive and Behavioural Practice. 10, 4, pp303-312
Children’s Commissioner for England (2015) Children in Care ad Care Leavers Survey 2015. London: Office of the Children’s Commissioner file:///C:/Users/June/Documents/Children%20dcsf/Chns%20commissioner %20LAC1Care%20monitor%20v12.pdf accessed 1.11.15
Dance, C., Ouwejan, D., Beecham, J. & Farmer, E. R. G. (2010) Adoption Agency Linking and Matching: a survey of adoption agency practice in England and Wales, London: BAAF
Farmer, E., Sturgess W., O’Neill T. and Wijedasa D. (2011) Achieving Successful Returns from Care: What makes reunification work?, London, BAAF
Featherstone, B., White, S. and Morris, K. (2014) Re-imagining child protection: towards humane social work with families, Bristol, The Policy Press.
Fernandez EA, (2012), Accomplishing Permanency: Reunification Pathways and Outcomes for Foster Children,, Springer, New York
Fernandez, E. and Barth, R. P.(2010) (eds) How does foster care work? London: Jessica Kingston pp 29-43
Fernandez, E. and Lee, J.S. (2011). ‘Returning children in care to their families: factors associated with the speed of reunification." Child Indicators Research, 4(4), pp 749-765
Gilbert, N., Parton, N. and Skivenes, M. (2011) Child Protection Systems: International Trends and Orientations Oxford, UK: Oxford University Press
Hansson, K., Olsson, M. (2012) ‘Effects of multidimensional treatment foster care (MTFC). Results from a RCT Study in Sweden’ Children and Youth Services Review, Vol 34, 9, pp 1929-1936
Maslow, A (1954). Motivation and personality. New York, NY: Harper.
Moffatt, P. and Thoburn, J. (2001) Outcomes of permanent family placement for children of minority ethnic origin.’ Child and Family Social Work, 6 (1) pp 13-22,
Neil, E., Beek, M., Ward, E. (2014) Contact after Adoption: A longitudinal study of adopted young people and their adoptive parents and birth relatives London: BAAF
Rowe, J., Hundleby, M. and Garnett, L. (1989) Child care now – a survey of placement patterns. London: BAAF.
Schofield, G. (2003) Part of the Family: Pathways through Foster Care. London: BAAF
Schofield, G., Beek, M. (2009) Growing up in foster care: providing a secure base through adolescence. Child & Family Social Work 14. pp. 255-266
Schofield, G. (ed.), Simmonds, J. (ed.) (2009) The Child Placement Handbook: Research, Policy and Practice
Schofield, G., Beek, M., Ward, E., Biggart, L. (2013) Professional foster carer and committed parent: Role conflict and role enrichment at the interface between work and family in long-term foster care In : Child and Family Social Work 18. pp. 46-56
Sebba, J., Berridge, D., Luke, N., Fletcher, J., Bell, K., Strand, S., Thomas, S., Sinclair, I. O’Higgins, A. (2015) The educational progress of looked after children in England. Oxford: Rees Centre
Sinclair, I., Baker, C., Lee, J. and Gibb, I. (2007) The Pursuit of Permanence. A Study of the English Child Care System
Skivenes, M. and Thoburn, J. (2016) Pathways to permanence in England and Norway: A critical analysis of documents and data. In Children and Youth Services Review 67, pp 152-160.
Thoburn, J. (1994) Child Placement: Principles and Practice. 2nd Edition, Aldershot: Ashgate
Thoburn, J. (2010a) ‘Achieving safety, stability and belonging for children in out-of-home care. The search for ‘what works’ across national boundaries’ International Journal of Child and Family Welfare Vol 12, Number 1-2 pp 34-48
Thoburn, J. (2010b) 'International Perspectives on Foster Care' in E. Fernandez and R.P. Barth. (eds) How does foster care work? London: Jessica Kingston pp 29-4
Thoburn, J. (2013) ‘Services for Vulnerable and Maltreated Children’ in I. Wolfe and M. McKee (eds.) European Child Health Services and Systems: Lessons without borders. Maidenhead: Open University Press/McGraw Hill
Thoburn, J. and Courtney, M. (2011) ‘A Guide through the knowledge base on children in out-of-home care’ Journal of Children’s Services, 6.4, 210-227
Thoburn, J., Robinson, J. and Anderson, B. (2012) Returning Children from Public Care. London: Social Care Institute for Excellence Research Briefing 42. http://www.scie.org.uk/publications/briefings/briefing42/
United Nations (1989) Convention on the Rights of the Child. New York: UN
Wade, J., Biehal, N., Farrelly, N. and Sinclair, I. (2011) Caring for Abused and Neglected Children: Making the Right Decisions for Reunification or Long-term Care, London, Jessica Kingsley.
Author´s
Address:
Emeritus Professor June Thoburn
School of Social
Work, UEA
Norwich, NR4 7TJ
email:
j.thoburn@uea.ac.uk
website
www.uea.ac.uk/swk/people